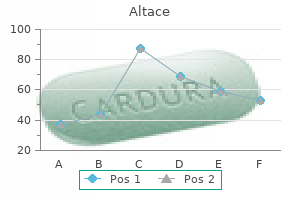
Buy 10 mg altace otcEvaluation of the Patient With Pulmonary Disease n 51 corresponding to carbolfuchsin or auramine-rhodamine pulse pressure is calculated by quizlet altace 2.5 mg order with mastercard, and the organisms are virtually distinctive of their capacity to retain the stain after acid is added heart attack exo altace 10 mg generic overnight delivery. Hence, the expression acid-fast bacilli is used commonly when referring to mycobacteria. Frequently used staining strategies are the Ziehl-Neelsen stain or a modification called the Kinyoun stain. A extra sensitive and faster way to detect mycobacteria includes use of a fluorescent dye corresponding to auramine-rhodamine. Mycobacteria take up the dye and fluoresce and may be detected comparatively simply even when current in small numbers. Because mycobacteria grow slowly, they may require 6 to eight weeks for development and identification on culture media. More lately, genetic probes have been employed to establish the presence of specific mycobacterial species with a lot larger speed and precision (see later). However, culture is usually nonetheless carried out to confirm the initial genetic test results and to allow drug sensitivity testing. Organisms apart from the widespread bacterial pathogens and mycobacteria usually require different specialized staining and culture strategies. Fungi may be recognized by special stains, corresponding to methenamine silver or periodic acid�Schiff stains, applied to tissue specimens. Cytologic examination for malignant cells is out there for expectorated sputum, specimens obtained by needle aspiration, bronchial washings or brushings obtained with a bronchoscope, and pleural fluid. A specimen could be smeared immediately onto a slide (as with a bronchial brushing), subjected to focus (bronchial washings, pleural fluid), or digested (sputum) previous to being smeared on the slide. The slide is then stained by the Papanicolaou approach, and the cells are examined for findings suggestive or diagnostic of malignancy. Pathologic examination of tissue sections obtained by biopsy is most useful for prognosis of malignancy or an infection, in addition to for quite lots of other processes affecting the lungs and pleura. In many circumstances, examination of tissue obtained by biopsy is the gold normal for analysis, although even biopsy outcomes can show false-negative findings or yield misleading info. Tissue obtained by biopsy is routinely stained with hematoxylin and eosin for histologic examination. A extensive assortment of other stains is on the market that more or less particularly stain collagen, elastin, and a selection of microorganisms. Further discussion of the specific strategies and stains can be found in standard pathology textbooks. Recently, state-of-the-art molecular biology techniques have been utilized to respiratory specimens for diagnosis of sure types of respiratory tract an infection. When in contrast with conventional culture methods, some nice benefits of molecular methods embody speedy detection and specific identification of pathogens, as properly as minimizing the hazard to laboratory personnel of publicity to rising pathogens. In addition, oligonucleotide hybridization probes enable speedy identification 52 n Principles of Pulmonary Medicine of organisms that have been cultured from scientific specimens. These newer molecular strategies have gotten more readily available and have seen rising scientific use over time. This final facet of analysis adds an essential dimension to total patient assessment as a outcome of it reflects how much the illness could restrict every day activities. In addition, a wide selection of measurements taken during train may help decide how a lot exercise a affected person can perform and what components contribute to any limitation of train. Pulmonary Function Tests Pulmonary perform testing provides an goal technique for assessing practical adjustments in a patient with known or suspected lung disease. With the results of exams which would possibly be broadly available, the doctor can answer several questions: (1) Does the affected person have important lung illness sufficient to trigger respiratory impairment and account for his or her signs Information obtained from such objective analysis may be essential in deciding when to deal with a affected person with lung illness and in assessing whether or not a affected person has responded to remedy. Preoperative evaluation of patients can be helpful in predicting which patients are more likely to have significant postoperative respiratory issues and that are prone to have adequate pulmonary function after lung resection. Three main categories of knowledge may be obtained with routine pulmonary function testing: 1. Lung volumes, which give a measurement of the size of the assorted compartments within the lung 2. Left, Block diagrams present two ways by which complete lung capability can be subdivided. To quantify these volumes, a selection of strategies can measure one of many three volumes, and the other two can then be calculated or derived from the spirometric tracing. Dilution checks: A identified quantity of an inert gasoline (usually helium) at a recognized concentration is inhaled into the lungs. This gasoline is diluted by the volume of fuel already current throughout the lungs, and the concentration of expired fuel (relative to inspired) subsequently reflects the initial volume of gasoline within the lungs. Body plethysmography: the affected person, sitting inside an hermetic field, performs a maneuver that causes growth and compression of gasoline throughout the thorax. In many circumstances, dilution methods are enough for figuring out lung volumes. Diffusing Capacity the diffusing capability is a measurement of the rate of switch of gasoline from the alveolus to hemoglobin inside a capillary, measured in relation to the driving stress of the fuel throughout the alveolar-capillary membrane. Carbon monoxide combines readily with hemoglobin, and the rate of switch of fuel from the alveolus to the capillary is determined by motion through the alveolar-capillary membrane and the amount of hemoglobin obtainable for binding the carbon monoxide. The measurement obtained throughout a diffusing capability test is primarily depending on the variety of functioning alveolar-capillary units-that is, the surface area obtainable for gas exchange-and the volume of blood (hemoglobin) in the pulmonary capillaries out there to bind carbon monoxide. Despite the name, as the test is carried out in scientific apply, the affect of the thickness of the alveolar-capillary membrane on the measured worth is actually minimal. Because the uptake of carbon monoxide by hemoglobin relies on the hemoglobin concentration in the blood, patients with anemia might have a depressed diffusing capacity measurement even if the lungs are regular. In practice, the diffusing capacity is often decreased in three categories of illness by which floor area for gas change is misplaced, pulmonary capillary blood quantity is decreased, or both: (1) emphysema, (2) diffuse parenchymal lung illness, and (3) pulmonary vascular disease. In disorders that have an result on solely the airways and not pulmonary parenchymal tissue. On the opposite hand, the diffusing capability could also be elevated in circumstances of latest Evaluation of the Patient With Pulmonary Disease n fifty five intrapulmonary hemorrhage on account of uptake of carbon monoxide by hemoglobin within the erythrocytes inside the alveolar spaces. Interpretation of Normality in Pulmonary Function Testing Interpretation of pulmonary perform tests necessarily entails a qualitative judgment about normality or abnormality on the premise of quantitative information obtained from these exams. Separate regression equations for women and men have been constructed to match the information obtained from these normal control topics. Separate race/ethnicity-specific equations are sometimes used due to slight variations in pulmonary perform in regular people of various races and ethnicities. Although the intent is to guarantee comparability of each individual to a related regular normal, the utility of race/ethnicity-specific equations has just lately been questioned and can be problematic for people with combined racial/ ethnic backgrounds. The requirements for determining what constitutes the "decrease limits of regular" for a specific take a look at range amongst laboratories. Most laboratories now consider values beneath the bottom 5th percentile of a standard reference group (also called the "95% confidence interval") to be abnormal, whereas others contemplate an noticed worth to be abnormal whether it is less than 80% of the anticipated worth. No matter which standards are used, all the info must be considered to determine whether certain patterns are constantly present.
Altace 10 mg buy generic lineCell-seeded or cell-free seeded scaffolds are able to rising bladder volume in small animals after hemi-cystectomy arrhythmia vs atrial fibrillation cheap 10 mg altace otc, whereas cell-seeded scaffolds are sometimes designed to substitute diseased bladder in a larger animal model after subtotal cystectomy pulse pressure range normal altace 2.5 mg order mastercard. A rodent model such as rat is often used to take a look at new cell sources or new biomaterials and examine histologic modifications within the regenerative bladder. Larger animal models are used to evaluate further the alterations in bladder function and volume, and anatomic and histologic structures (Table seventy two. Beagles or minipigs are mostly used larger animal models for these purposes. Fibrotic Bladder Model Most in vivo experiment models of tissue engineered bladders are carried out in the regular bladder after cystectomy. However, in medical conditions, sufferers have diseased bladders with fibrosis or persistent inflammation or lack a good blood supply. Thus, a mannequin is needed that mimics illness circumstances to take a look at the potential of tissue engineering know-how. Several approaches have been used to create a neurogenic bladder dysfunction mannequin [103] or fibrotic bladder mannequin induced by bladder atrophy owing to urinary diversion [104], bladder ischemia [105], or chemical brokers [106]. To generate a bladder atrophy model, urinary diversion is performed to trigger a speedy decrease in contractile function in adult or fetal animal bladders. Female SpragueDawley rats had been distributed into age matched control, sham urinary diversion and urinary diversion groups. Each group was subsequently evaluated 1 or 8 weeks after urinary diversion or sham operation. Diversion was carried out by surgical disconnection of the ureters from the bladder and implantation into the uterine cervix. Smooth muscle and urothelium have been decreased as a proportion of the total bladder cross-sectional area. Collagen increased in rats with either 1 or eight weeks of urinary diversion versus controls. Urinary diversion caused decreased expression of muscarinic 3 and ligand-gated purinergic 1 receptor but no change in muscarinic 2 or ligand gated purinergic 2 receptors. Urinary diversion causes dysfunctional and irregular morphometric alterations in the bladder in this mannequin. Bladders from fetal sheep subjected to urinary diversion weighed considerably less than management fetal bladders. Marked reorganization of clean muscle parts was observed in those with diversion. Contractile responses of defunctionalized strips to carbachol were significantly lower than those of management bladder strips. In transient, urinary diversion in regular fetal sheep resulted in marked bladder atrophy, decreased muscle mass, and decreased bladder contractility. Both indwelling urethral catheterization and suprapubic catheterization are forms of urinary diversion. The former is related to a threat for urolithiasis, urethral trauma, urethral erosions and/or strictures, bladder fibrosis, epididymitis, orchitis, and bladder cancer. Therefore, in most clinical cases, indwelling urethral catheters are inappropriate for long-term treatment and suprapubic catheters are a better possibility. However, medical data [108] showed that long-term indwelling urinary catheterization has comparable charges of higher tract harm, vesicoureteral reflux, renal or bladder calculi, and symptomatic urinary tract infections in contrast with suprapubic catheters. The catheter was changed every 2 weeks, which might stop the problems of indwelling urethral catheterization. Histologic analysis indicated that viable cells had been in a position to self-assemble again into their respective tissue types and would retain their native phenotype [109]. These experiments demonstrated for the first time that composite layered tissue engineered constructions could be created de novo. Before this research, only nonlayered constructions had been created in the area of regenerative drugs. To determine the effects of implanting engineered tissues in continuity with the urinary tract, animal fashions of bladder augmentation have been used [110]. One group had the bladder augmented with a nonseeded bladder-derived collagen matrix; the second group had the bladder augmented with a cell-seeded construct. The bladders augmented with matrices seeded with cells confirmed a 100 percent enhance in capacity compared with bladders augmented with cell-free matrices, which showed solely a 30% improve in capability. Most of the free grafts (without cells) used for bladder replacement in the past were able to show sufficient histology by method of a well-developed urothelial layer, however they have been associated with an irregular muscular layer that diversified by method of its full improvement. It has been well-established for decades that the bladder is prepared to regenerate generously over free grafts. Both urothelial and muscle ingrowth are believed to be initiated from the sides of the traditional bladder toward the region of the free graft [111]. The inflammatory response toward the matrix could contribute to the resorption of the free graft. It was hypothesized that building 3D construction constructs in vitro before implantation would facilitate the eventual terminal differentiation of the cells after implantation in vivo and decrease the inflammatory response towards the matrix, thus avoiding graft contracture and shrinkage. The canine study demonstrated a significant difference between matrices used with autologous cells (tissue engineered matrices) and those used without cells [110]. Matrices implanted with cells for bladder augmentation retained most of their implanted diameter, versus matrices implanted with out cells for bladder augmentation, during which graft contraction and shrinkage occurred. The histomorphology demonstrated a marked paucity of muscle cells and a more aggressive inflammatory reaction in matrices implanted without cells. Epithelial mesenchymal signaling is important for the differentiation of bladder clean muscle [112]. To tackle the functional parameters of tissue engineered bladders higher, an animal mannequin was designed that required a subtotal cystectomy with subsequent substitute with a tissue engineered organ [113]. Cystectomy-only and nonseeded controls maintained common capacities of 22% and 46%, respectively, of preoperative values. An common bladder capacity of 95% of the original precystectomy volume was achieved in the cellseeded tissue engineered bladder replacements. The compliance of the cell-seeded tissue engineered bladders showed almost no distinction from preoperative values that have been measured when the native bladder was current (106%). The retrieved tissue engineered bladders confirmed a traditional cellular group consisting of a trilayer of urothelium, submucosa, and muscle. The technique of utilizing biodegradable scaffolds with cells may be pursued with out considerations concerning local or systemic toxicity [115]. However, not all scaffolds perform properly if a big portion of the bladder wants alternative. The use of bioreactors, during which mechanical stimulation is started at the time of organ production, has also been proposed as an important parameter for fulfillment [117,118]. To consider the impact of cell-seeded tissue engineering technology within the bladder regeneration compared with scaffold alone, a gaggle of experimental canines underwent a trigone-sparing cystectomy and have been randomly assigned to one of three groups. The cystectomy-only and nonseeded controls maintained common capacities of 22% and 46%, respectively, of preoperative values. The compliance of the cell-seeded tissue engineered bladders was nearly no completely different from preoperative values (106%).
Cheap 5 mg altace mastercardThe elastic design of those retractors theoretically reduces the chance for compressive nerve harm associated with metallic retractor blades; nonetheless pulse pressure product order 10 mg altace with visa, evidence is solely anecdotal hypertension quality improvement trusted altace 5 mg. The nerves most prone to dissection-related damage embrace the obturator and, much less generally, the femoral nerve. Obturator nerve trauma is extra generally encountered in oncological surgical procedure but can be a sequelae to surgery for deep infiltrating endometriosis as nicely. Recognition Clinically, sufferers with femoral neuropathy current with motor deficits, similar to weakness or incapability to flex on the hip or to prolong at the knee, and can even complain of impaired sensory operate involving paresthesias over the anterior and medial thigh as properly as the medial side of the calf. Patients will complain of both sensory or motor deficits representing the distribution of the injured nerve. Further particulars may be found in the "Postoperative Neuropathy" section beneath General Issues. Depending on the physical limitations ensuing from the deficit, a neurology session may be required as properly. In a prospective study of over 600 ladies present process gynecologic surgery, 12 patients (1. A thorough understanding of the prognosis and management of surgical problems is critical. Cardiopulmonary physiology and pathophysiology as a consequence of laparoscopic surgery. Variables related to postoperative deep venous thrombosis: a prospective examine of 411 gynecology patients and creation of a prognostic mannequin. Laparoscopic surgery is associated with a lower incidence of venous thromboembolism compared with open surgery. Risk of venous thromboembolism in belly versus minimally invasive hysterectomy for benign conditions. Predictors of surgical website an infection in ladies present process hysterectomy for benign gynecologic illness: a multicenter evaluation utilizing the nationwide surgical high quality enchancment program knowledge. Does pre- and postoperative metronidazole therapy lower vaginal cuff infection rate after stomach hysterectomy amongst women with bacterial vaginosis Tuboovarian abscesses: is size associated with duration of hospitalization and issues Incidence and affected person traits of vaginal cuff dehiscence after completely different modes of hysterectomies. Vaginal cuff closure after minimally invasive hysterectomy: our experience and systematic review of the literature. Incidence and traits of patients with vaginal cuff dehiscence after robotic procedures. Comparison of woundhealing characteristics with feedback circuit electrosurgical generators in a porcine model. Histologic characteristics of vaginal cuff tissue from sufferers with vaginal cuff dehiscence. Incidence, risk components and morbidity of unintended bladder or ureter damage during hysterectomy. Accuracy of cystoscopy in the diagnosis of ureteral harm in benign gynecologic surgery. Prevention, recognition, and management of urologic accidents throughout gynecologic surgery. Conservative administration of incidental cystotomy at laparoscopy: a report of two cases. A case-control research of threat elements for ileus and bowel obstruction following benign gynecologic surgery. Adhesion barrier use after myomectomy and hysterectomy: rates and immediate postoperative issues. A randomized, managed examine evaluating minilaparotomy versus isobaric gasless laparoscopic assisted minilaparotomy myomectomy for removal of huge uterine myomas: short-term outcomes. Uterine myomectomy: function of gasless laparoscopy in comparison with other minimally invasive approaches. Gasless laparoscopic surgery during pregnancy: analysis of its role and usefulness. Role of microlaparoscopy within the prognosis of peritoneal and visceral adhesions and in the prevention of bowel harm associated with blind trocar insertion. Safe entry strategies during laparoscopy: left higher quadrant entry using the ninth intercostal space-a evaluation of 918 procedures. Preoperative ultrasound to predict infraumbilical adhesions: a research of diagnostic accuracy. Office visceral slide check in contrast with two perioperative exams for predicting periumbilical adhesions. Impact of obstructive sleep apnea on lung volumes and mechanical properties of the respiratory system in overweight and obese individuals. Longer operative time during benign laparoscopic and robotic hysterectomy is related to increased 30-day perioperative problems. Intraocular stress during robotic-assisted laparoscopic procedures using steep Trendelenburg positioning. The effect of dilute vasopressin answer on blood loss throughout operative hysteroscopy. Preventing hyponatremic encephalopathy: comparison of serum sodium and osmolality throughout operative hysteroscopy with 5. A combination of misoprostol and estradiol for preoperative cervical ripening in postmenopausal ladies: a randomised managed trial. Effectiveness of estrogen within the prevention of intrauterine adhesions after hysteroscopic septal resection: a prospective, randomized examine. Efficacy of estrogen therapy in sufferers with intrauterine adhesions: systematic evaluate. Anti-adhesion barrier gels following operative hysteroscopy for treating female infertility: a systematic review and meta-analysis. Reproductive outcomes after operative hysteroscopy utilizing sodium hyaluronate and carboxymethylcellulose. The incidence of urinary tract harm during hysterectomy: a prospective evaluation based mostly on universal cystoscopy. Management of ureteral accidents associated with vaginal surgical procedure for pelvic organ prolapse. Is earlier cesarean section a danger for incidental cystotomy on the time of hysterectomy Anatomic relationships of the distal third of the pelvic ureter, trigone, and urethra in unembalmed feminine cadavers. Urinary tract injury at benign gynecologic surgery and the role of cystoscopy: a scientific review and metaanalysis.
Purchase altace 2.5 mg overnight deliveryTheir cytoplasm incorporates a wide selection of Lung Defense Mechanisms n 289 granules of varied styles and sizes medication to lower blood pressure quickly 2.5 mg altace order amex, lots of which are packages of digestive enzymes that can get rid of ingested international materials arteria 23 generic altace 2.5 mg with mastercard. Alveolar macrophages have a serious role in killing microorganisms that have reached the lower respiratory tract. They also launch chemoattractant cytokines (chemokines) that recruit different inflammatory cells. When an alveolar macrophage is uncovered to inhaled particles or micro organism, attachment of the overseas materials to the surface of the macrophage is the primary step within the processing sequence. The particles or bacteria are engulfed throughout the plasma membrane, which invaginates and pinches off throughout the cell to type a cytoplasmic phagosome containing the now isolated international materials. In some circumstances, this sequence of attachment and phagocytosis is facilitated by opsonins, which coat the international materials. Opsonins are proteins that bind to extracellular materials and make them more adherent to phagocytic cells and extra amenable to engulfment or ingestion. Opsonins can be particular for the actual foreign substance, corresponding to antibodies directed towards antigenic material, or they might demonstrate nonspecific binding to quite lots of substances. Particularly essential specific opsonins are antibodies of the IgG class directed against antigenic international material, either bacteria or different antigenic particles. Nonspecific opsonins in the lung include secretory IgA, complement, and fibronectin. After micro organism or different international materials is isolated inside phagosomes, a process of intracellular digestion occurs throughout the macrophage. Often the phagosomes combine with lysosomes to form phagolysosomes, by which proteolytic enzymes supplied by the lysosome digest, detoxify, or destroy the phagosomal contents. In addition to lysosomal enzymes, a variety of oxidation products, corresponding to hydrogen peroxide and different intermediate merchandise of oxidative metabolism, are poisonous to bacteria and play a role within the capacity of the macrophage to kill ingested microorganisms. Macrophages launch inflammatory mediators such as tumor necrosis factor- and interleukin-1, as nicely as different cytokines and chemokines that are energetic in recruiting further inflammatory cells. In some cases, similar to with inhaled silica particles, the ingested materials is toxic to the macrophage and finally could kill the phagocytic cell. An more and more appreciated function of the alveolar macrophage is to suppress irritation in the lung. Even a small amount of inflammation inside the alveolar wall would have a negative effect on gasoline change, and a fantastic steadiness retains the distal airways freed from infection, however not in a state of constant harmful irritation. Alveolar macrophages are capable of course of a considerable quantity of inhaled substances with out inciting an immune response exterior to the macrophage itself. It is estimated that the traditional pool of alveolar macrophages can handle as much as 109 inhaled micro organism earlier than the bacteria overwhelm the macrophages and trigger infection within the alveoli. In addition, alveolar macrophages, via complicated signaling mechanisms, function to maintain dendritic cell and T cell activation in verify. The detailed working of this fantastic equilibrium between irritation and quiescence within the lung is an space of active analysis. They are bonemarrow� derived cells that, in the lung, are situated within the airway epithelium as properly as in alveolar Major phagocytic and resident inflammatory cells are: 1. Natural killer cells 290 n Principles of Pulmonary Medicine partitions and peribronchial connective tissue. These cells have long and irregular cytoplasmic extensions that kind a contiguous community. The main operate of dendritic cells is to pattern the airway microenvironment, ingest and course of antigens, after which migrate to regional lymph nodes. In the lymph nodes, dendritic cells present antigen to T cells, a critical step for the later immunologic defense provided by lymphocytes. Langerhans cells, a type of dendritic cell with a selected ultrastructural appearance, are the cells with irregular proliferation that seem to be answerable for Langerhans cell histiocytosis of the lung (also called eosinophilic granuloma; see Chapter 11). When micro organism overwhelm the preliminary defense mechanisms already mentioned, they might replicate within alveolar areas, inflicting a bacterial pneumonia. These cells most likely are attracted to the lung by a variety of stimuli, significantly merchandise of complement activation and chemotactic components released by alveolar macrophages. Neutrophil granules include several antimicrobial substances, including defensins, lysozyme, bacterial permeability�increasing protein, and lactoferrin. In addition, neutrophils can generate merchandise of oxidative metabolism which are poisonous to microbes. They act by recognizing and killing virus-infected cells which have been reworked and now not specific certain markers of cellular well being on the cell floor. Bacteria, viruses, and different microorganisms are perhaps an important antigens to which the respiratory tract is repetitively uncovered. Presumably, immune protection mechanisms are particularly essential in defending the person against these agents. For more detailed information, the reader is referred to specialised texts and evaluation articles on immunology. The two major components of the adaptive immune system are humoral (or B-lymphocyte related) and mobile (or T-lymphocyte related). Cellular immunity refers to the activation of T lymphocytes (which depend on the thymus for differentiation) and the execution of certain particular T-lymphocyte features, including the production of soluble mediators or cytokines. In explicit, T lymphocytes seem to have an important function in regulating immunoglobulin or antibody synthesis by the humoral immune system. Both humoral and cellular immunity are necessary in the protection of the respiratory system towards microorganisms. For sure infectious agents, humoral immunity is the first mode of safety. In the lung and in blood, T lymphocytes are more numerous than B lymphocytes, but both systems are essential for efficient protection against the spectrum of doubtless dangerous microorganisms. Lymphocytes could be discovered in many places within the respiratory tract, extending from the nasopharynx all the way down to distal areas of the lung parenchyma. True lymph nodes are present around the trachea and carina, and on the hilum of every lung in the region of the mainstem bronchi. These lymph nodes obtain lymphatic drainage from most of the airways and lung parenchyma. Lymphoid tissue is current in the nasopharynx, and collections of lymphocytes arranged in nodules are found along medium to massive bronchi. These latter collections are called bronchus-associated lymphoid tissue and could also be responsible for intercepting and handling antigens deposited alongside the conducting airways. Smaller aggregates of lymphocytes could be discovered in additional distal airways and even scattered all through the pulmonary parenchyma. Humoral Immune Mechanisms Humoral immunity in the respiratory tract seems within the type of two major courses of immunoglobulins: IgA and IgG. Antibodies of the IgA class are significantly important in the nasopharynx and upper airways, where they constitute the primary antibody kind. The type of IgA current in these areas is secretory IgA, which features a dimer of IgA molecules (joined by a polypeptide) plus an additional glycoprotein element termed the secretory element. Secretory IgA appears to be synthesized regionally, and the quantities of IgA are a lot larger in the respiratory tract than within the serum.
Altace 5 mg generic with mastercardFatigued respiratory muscles are allowed to recover hypertension 6 year old 10 mg altace cheap free shipping, and the comparatively large amount of blood move required by overworking respiratory muscle tissue may be shifted to perfusion of different organ systems hypertension nursing assessment 2.5 mg altace effective. Reducing the work of breathing is a advantage of mechanical ventilation in all forms of acute respiratory failure. By supporting fuel trade and assisting with the work of air flow for as lengthy a interval as essential, mechanical ventilators can keep a affected person alive whereas the acute process precipitating respiratory failure is handled or allowed to resolve spontaneously. This part briefly describes the operation of mechanical ventilators, the available modes of ventilation, and the problems that may ensue from their use. Ventilators at present used for management of acute respiratory failure are positivepressure units: they deliver fuel beneath positive strain throughout inspiration. However, the ventilator settings are sometimes fairly completely different, depending upon the type of respiratory failure. Pressure-Limited Ventilation Two kinds of pressure-limited air flow are used generally in sure medical settings. This degree of stress help is reached quickly and maintained all through most of inspiration. The volume 374 n Principles of Pulmonary Medicine With volume-cycled air flow, inspiration terminates after a specified tidal volume has been delivered by the ventilator. With pressure-limited ventilation, inspiration terminates after the focused airway strain has been achieved. However, changes in lung compliance and airway resistance do alter the quantity of gasoline delivered as the desired target stress is reached. Volume-Cycled Ventilation When the ventilator is used in a volume-cycled fashion, each inspiration is terminated (and passive expiration allowed to occur) after a specified volume has been delivered by the machine. Volume cycling is much more dependable than pressure-limited air flow in delivering constant, specified tidal volumes. However, the stress required to deliver a particular quantity will range depending on lung compliance and airway resistance and may change over time as these parameters get higher or worse. In managed ventilation, air flow is equipped totally by the ventilator at a respiratory fee, tidal volume, and inspired O2 concentration chosen by the physician. In the assist-control mode of ventilation, the ventilator is ready to "sense" when the patient initiates inspiration, at which point the machine assists by delivering a specified tidal volume. Although the tidal quantity is set by the machine, the respiratory price is decided by the variety of spontaneous inspiratory efforts made by the patient. For example, if the backup rate set on the machine is 10 breaths/min, the ventilator will automatically deliver a breath if and when 6 seconds have elapsed from the previous breath. In this example, if the affected person is spontaneously initiating breaths at 16 breaths/ min, all breaths are triggered by the patient. Airway pressure during spontaneous air flow and during mechanical ventilation with several totally different ventilatory patterns. Relative timing of inspiration and expiration is managed by physician-determined ventilator settings. However, if the expiratory portion of the tubing is linked to a valve requiring a pressure of no much less than 10 cm H2O, for instance, to open it, the valve closes and expiration ceases when the airway stress falls to 10 cm H2O. Although no positive stress is offered by a mechanical ventilator during inspiration, inspired gasoline is delivered from a reservoir bag under tension or at a sufficiently excessive move price to hold airway pressure optimistic during inspiration as properly as expiration. Important targets of these specific strategies are to forestall closure of alveoli throughout expiration while concurrently avoiding supply of excessive volume and pressure to the airways and alveoli, with the potential for secondary issues (see later). In some instances, Pco2 may rise when these comparatively low tidal volumes are used, but the elevation in Pco2 above regular ranges is considered an appropriate strategy of permissive hypercapnia. By minimizing the need for prime ventilation requirements, this technique theoretically decreases the risks of developing excessive alveolar pressures and overdistention and harm of some alveolar models. Prone positioning can enhance oxygenation, improve clearance of secretions, and reduce ventilator-induced lung harm. An adjunctive remedy that will improve oxygenation however has not been proven to enhance survival is the utilization of inhaled pulmonary vasodilators, corresponding to nitric oxide (a gas) or epoprostenol (an aerosol). Because these medications are delivered via inhalation, they preferentially journey to the extra ventilated alveoli and enhance relative blood flow to these better-functioning lung models. Local vasodilation in these lung models results in improved ventilation-perfusion matching and a higher Po2 in blood getting back from the lungs to the left facet of the guts. Discontinuation of Ventilatory Support When the underlying problem that precipitated the need for mechanical air flow has improved, ventilatory help is discontinued, sometimes after observing the patient throughout a short (30 to one hundred twenty minutes) trial of spontaneous respiration with minimal or no optimistic stress delivered by the mechanical ventilator. Although the time period weaning remains to be applied to discontinuation of mechanical air flow, the older technique of slowly lowering the amount of support offered by the ventilator is mostly now not used. As rational as it appears to wean the patient gradually from ventilatory support, another and superior strategy is to carry out an empiric day by day trial of spontaneous breathing. Noninvasive Ventilatory Support for Acute Respiratory Failure When patients with acute respiratory failure require mechanical air flow, assist traditionally has been offered by constructive strain administered through a tube positioned into the trachea. However, use of the tube is related to risks and issues, such as patient discomfort from the tube itself, damage to the larynx or trachea, and development of lower respiratory tract infection (Table 29. High-flow (up to 60 L/min) warmed, humidified oxygen delivered via large nasal prongs could also be another choice to avoid endotracheal intubation in patients with less extreme forms of acute hypoxemic respiratory failure. Complications of Intubation and Mechanical Ventilation Intubation and mechanical ventilation of sufferers in respiratory failure are associated with potential risks and problems (see Table 29. Mechanical air flow could be discontinued after a profitable trial of spontaneous respiration. When a tube remains in the trachea for days to weeks, problems affecting the larynx and trachea can happen. The trachea is subject to ulcerations, stenosis, and tracheomalacia (degeneration of supporting tissues within the tracheal wall) resulting from pressure applied by the inflated balloon on the end of the tube. As a precaution to lower tracheal problems, tubes are made with cuffs that minimize the pressure exerted on the tracheal wall and the ensuing pressure necrosis. For prolonged ventilatory assist (weeks to months), a tracheostomy tube positioned instantly into the trachea via an incision within the neck has some advantages over extended orotracheal or nasotracheal intubation, including affected person consolation and prevention of additional vocal wire harm. The presence of an endotracheal tube puts the patient at significant risk for nosocomial pneumonia, usually referred to as ventilator-associated pneumonia. They embrace bypassing of the normal anatomic barriers and higher airway clearance mechanisms that forestall organisms from reaching the lower respiratory tract, aspiration of oropharyngeal secretions across the endotracheal tube and into the lower respiratory tract, and bacterial contamination of the endotracheal tube or the ventilator circuitry connected to the endotracheal tube. Organisms inflicting ventilator-associated pneumonia are sometimes comparatively antibiotic-resistant bacteria, including gram-negative bacilli and Staphylococcus aureus, resulting in important increases in each period of hospitalization and mortality. Administration of positive strain by a mechanical ventilator has its own attendant problems. Patients receiving positive-pressure air flow are subject to barotrauma- traumatic adjustments such as pneumothorax or pneumomediastinum occurring as a end result of excessive alveolar pressures. Because alveolar overdistention with rupture is at present thought to be the cause for these complications, the term volutrauma is now usually used as a substitute of barotrauma. Development of a pneumothorax in patients receiving mechanical ventilation can have catastrophic consequences if not detected and treated Management of Respiratory Failure n 379 shortly. The ventilator continues to ship fuel underneath positive pressure, and the gasoline enters the pleural area via the rupture.
Altace 2.5 mg order with visaIn the case of close to drowning in either recent or salt water hypertension and stroke order 5 mg altace, not only does the inhaled water fill alveolar areas heart attack 1 hour cheap 10 mg altace fast delivery, however secondary harm to the alveolar-capillary barrier causes fluid to leak from the pulmonary vasculature. Fresh water, then again, is hypotonic to plasma and mobile contents and thus could enter pulmonary parenchymal cells, with resulting cellular edema. In addition, recent water seems to inactivate surfactant, a complicating issue discussed in more detail under Pathophysiology. Finally, aspirated hydrocarbons may be toxic to the distal parenchyma, perhaps in Acute Respiratory Distress Syndrome n 361 Table 28. Nitrogen dioxide is one instance, as are some chemical products of combustion inhaled in smoke. A high focus of inhaled oxygen, particularly when given for prolonged intervals, contributes to alveolar injury. The mechanism of O2 toxicity is believed to be the generation of free radicals and superoxide anions, byproducts of oxidative metabolism which might be poisonous to pulmonary epithelial and endothelial cells. Infectious brokers may produce injury via airway entry to the pulmonary parenchyma. However, in most cases a specific circulating factor has not been identified with certainty, even though several possibilities have been proposed. When fats or amniotic fluid enters the circulation, the fabric is transported to the lungs, ensuing in the scientific issues of fats embolism and amniotic fluid embolism, respectively. One of the brokers most frequently acknowledged has been heroin, and the name "heroin pulmonary edema" generally is used. Some sufferers with acute pancreatitis develop a clinical image according to noncardiogenic pulmonary edema. In this example, enzymes launched into the circulation from the damaged pancreas have been proposed to directly injure pulmonary parenchymal cells or initiate different indirect pathways, leading to harm. An attention-grabbing and generally accepted speculation to clarify this so-called neurogenic pulmonary edema is that intense sympathetic nervous system discharge in response to intracranial hypertension produces vasospasm and extremely high pulmonary capillary pressures, leading to mechanical harm to the endothelium and subsequent exudation of fluid out of the intravascular area. One essential issue appears to be the ability to produce harm to pulmonary capillary endothelial and alveolar epithelial cells (primarily type I epithelial cells, the cytoplasmic processes of which give many of the surface space lining the alveolar walls). Given the wide variety of insults that may damage these cell types, it appears unlikely that a single common mechanism is operative for every kind of damage. Here the extra generalized cellular and biochemical mechanisms which are operative through the course of harm to the pulmonary epithelial and capillary endothelial cells are thought of. An early principle explaining recruitment of neutrophils to the lungs focused on the complement pathway. When complement is activated by sepsis, C5a is launched and is answerable for aggregation of neutrophils inside the pulmonary vasculature. These neutrophils may release a selection of substances which are probably damaging to cellular and noncellular elements of the alveolar wall. Superoxide radicals, other byproducts of oxidative metabolism, an array of cytokines, and numerous proteolytic enzymes all could be launched by neutrophils and could also be essential pathogenetically in producing structural and useful damage to the alveolar wall. Activation of complement is only one of multiple potential mechanisms for recruiting and sequestering neutrophils in the lungs. Other important elements embrace cytokines and other mediators that affect neutrophil trafficking in the lungs. Vascular endothelial cells, notably within the pulmonary vascular system, also turn into activated, express leukocyte adhesion molecules, and lead to accumulation of neutrophils within the pulmonary vasculature. Several components are answerable for what has been known as a "procoagulant state," together with release of procoagulant tissue components, a decreased focus of factors with anticoagulant activity. Further clarification of pathogenesis and the importance of varied pathways and mediators will be crucial to the development of effective types of prevention and remedy. Activation of the vascular endothelium and expression of leukocyte adhesion molecules three. Injury to kind I alveolar epithelial cells and pulmonary capillary endothelial cells appears to be the primary factor in pathogenesis. Type I epithelial cells incessantly appear necrotic and should slough from the floor of the alveolar wall. Damage to capillary endothelial cells is mostly more difficult if not inconceivable to recognize with light microscopy; electron microscopy could additionally be essential to recognize the delicate ultrastructural modifications. The lung parenchyma reveals an influx of inflammatory cells, both in the interstitial space and often in the alveolar lumen. The cellular response is comparatively nonspecific, consisting of neutrophils and macrophages. Hyaline membranes are composed of a mixture of fibrin, cellular debris, and plasma proteins which may be deposited on the alveolar surface. After approximately 1 to 2 weeks, the exudative phase evolves right into a proliferative phase. Another component of the proliferative section is accumulation of fibroblasts within the pulmonary parenchyma. Often accompanying the fibrosis are adjustments within the pulmonary vasculature, which embrace intensive transforming and compromise of the lumen of small vessels by intimal and medial proliferation and by the formation of in situ thrombi. The most striking problem is alveolar flooding, which effectively prevents air flow of affected alveoli, despite the fact that perfusion may be comparatively preserved. These alveoli, perfused but not ventilated, act as regions where blood is shunted from the pulmonary arterial to pulmonary venous circulation without ever being oxygenated. To some extent, this phenomenon outcomes from a nonuniform distribution of the pathologic course of inside the lungs. In areas where the interstitium is extra edematous or the place more fluid is current in the alveoli, air flow is extra impaired (even though some ventilation remains) than in areas which were relatively spared. In addition to the direct results of interstitial and alveolar fluid on oxygenation, other changes seem to be secondary to alterations within the manufacturing and effectiveness of surfactant. Chapter eight refers to surfactant as a mix of lipids, 4 specific proteins, and carbohydrates answerable for reducing floor pressure and sustaining alveolar patency. In addition, proof means that because of intensive fluid throughout the alveoli, surfactant is inactivated and due to this fact ineffective in preventing alveolar collapse. In terms of oxygenation, both ventilation-perfusion mismatch (with areas of low ventilation-perfusion ratio) and true shunt (ventilation-perfusion ratio = 0) contribute Acute Respiratory Distress Syndrome n 365 to hypoxemia. Insofar as shunt is responsible for a lot of the drop in Po2, supplemental O2 alone might not restore oxygenation to normal. In practice, Po2 does rise somewhat with administration of one hundred pc O2, but not nearly to the extent anticipated after such excessive concentrations of O2. Changes in Pulmonary Vasculature the pulmonary vasculature is topic to modifications resulting from the general pathologic process. Hypoxemia actually produces vasoconstriction throughout the pulmonary arterial system, and fluid in the interstitium could enhance interstitial pressure, leading to a lower in size and a rise in resistance of the small pulmonary vessels. The lumen of small vessels could also be compromised by microthrombi and proliferative adjustments in vessel partitions (discussed earlier under Pathogenesis and Pathology).
Diseases - Immotile cilia syndrome, Kartagener type
- Microcephaly cardiac defect lung malsegmentation
- Polyglucosan body disease, adult
- Locked-in syndrome
- Deafness symphalangism
- Lichen planus follicularis
- Narcissistic personality disorder
Order altace 2.5 mg on-lineOnce afebrile for twenty-four to forty eight hours arteriae rectae altace 2.5 mg cheap online, the affected person ought to be transitioned to oral drugs arrhythmia recognition posters discount altace 5 mg free shipping, such as metronidazole 500 mg each 12 hours and trimethoprim/sulfamethoxazole 160/800 mg every 12 hours or ampicillin/clavulanate 875/125 mg each 12 hours to complete a 14-day course. Should the location of the gathering be low within the pelvis, the transvaginal approach is preferred and could merely comprise bluntly opening the vaginal cuff and probing the abscess cavity to facilitate drainage. Uncommonly, laparoscopically or laparotomically directed drainage may be essential, assisted by intraoperative ultrasound as acceptable. Wound issues (excluding infection) Abdominal wound dehiscence and incisional hernia Wound dehiscence is acute postoperative lack of the integrity of the wound and, particularly, the fascial closure, a complication that normally manifests inside the first week after surgery. This separation of the fascial wound edges usually occurs secondary to one or a mix of circumstances including poor tissue quality, suture or knot failure, inadequate bites of fascial tissue, and stresses on the wound from coughing or vomiting. Incisional hernia is essentially a chronic wound failure with deterioration of the fascial integrity beneath an intact cutaneous layer and above an intact peritoneum. The risk of each hernia and stomach fascial dehiscence is decreased by employing correct approach, a process that begins with suture selection. For fascial closure, surgeons ought to keep away from utilizing all catgut sutures and slender caliber suture of any sort. Fascial closure is most appropriately performed utilizing a big caliber working monofilament (example 0 or No. In higher-risk circumstances, based on tissue quality or the chance of postoperative coughing or vomiting, a double strand of suture. For example, a randomized controlled trial evaluating hernia rates related to midline incisions after using small bites (tissue bites of 5 mm from the would edge and intersuture spacing of 5 mm) versus giant bites (1 cm � 1 cm) discovered fewer hernias in the small bites group (13% versus 21%). Vaginal cuff dehiscence the issue Vaginal cuff dehiscence is a serious potential complication of complete hysterectomy by way of any route but has been reported to be extra frequent with the laparoscopic approach. Despite this, vault dehiscence remained a rare event till the appearance of laparoscopic strategies. Risk-reducing measures A variety of investigators have proposed steps that might be taken to scale back the risk of vault dehiscence, particularly following laparoscopic hysterectomy. These embrace minimizing the use of energy-based tissue coagulation along and adjacent to the wound edge to that necessary for adequate hemostasis. The second is to ensure that, for whatever closure method used, the chew depth is enough to seize tissue not affected by the utilized power, maybe 10 mm. Patients should be instructed concerning pelvic rest; avoiding intercourse and heavy lifting for a minimal of 6 to 8 weeks. Recognition Vaginal cuff dehiscence could current with some mixture of pain, vaginal bleeding or discharge, and indicators and signs of vault infection. In the presence of evisceration, the examiner may visualize or palpate bowel within the vagina or by way of the introitus. Management Repair can normally be completed vaginally with 0 braided or other delayed absorbable suture using a working General issues a hundred sixty five or interrupted method based on the extent of the defect and surgeon preference. There may be value in trimming back the vaginal edges to facilitate obtaining suture purchase on viable tissue. The incidence of bladder harm at the time of whole stomach (laparotomic) hysterectomy has been reported to be 6. The web site of injury can range substantially and, because of the trail of dissection, could more generally involve the trigone. Ureteral harm Gynecologic patients are additionally in danger for ureteral damage, relying on the procedure performed, with one study suggesting a frequency of 1. For instance, the path of the ureter could be altered in sufferers with endometriosis where fibrosis and retraction of tissue usually result in medial deviation toward the uterosacral ligament, inserting it at larger danger of injury. Ovarian masses, notably endometriomas that are inclined to fuse to the lateral peritoneum, also bring the ureter closer to the zone of operative dissection. The vaginal approach may additionally be related to ureteric harm, notably during surgery for pelvic organ prolapse. In fact, in a sequence of 46 women present process bilateral uterosacral vaginal vault restore and site-specific restore of endopelvic fascial defects, 11% were difficult by ureteral harm. Similarly, it could be prudent to avoid suprapubic ancillary ports during laparoscopic procedures if it is suspected that the bladder is pulled or displaced in a rostral direction. When performing myomectomy, or especially hysterectomy in high-risk patients, intermittent partial filling of the bladder by occluding the outflow whereas instilling fluid via the third channel of the catheter can help outline appropriate and safe surgical planes. Having sufficient instrumentation to present sufficient traction and countertraction will regularly facilitate identification of the areolar plane that separates the bladder from the cervix. When performing vaginal surgical procedure close to the bladder, particularly hysterectomy and anterior colporraphy, additional steps could be thought-about. Ureter Pathology corresponding to endometriosis, more common on the left, or leiomyomas that extend into the cervix or broad ligament, can impact the course and identification of the ureters. The use of retroperitoneal identification and appropriate dissection to decide the anatomical course of the ureter is described in detail in Chapter 1. If one encounters surprising problem, a urologist or surgeon with appropriate training can place the stents after the dissection has begun. As properly, if the surgeon is uncomfortable or unfamiliar with ureteric dissection, arranging to have out there a urologic colleague or a gynecological surgeon with such experience can be a useful step. When performing hysterectomy, there are some ideas that should be observed whatever the chosen route: laparoscopic, laparotomic, or vaginal. For every, it could be very important perceive the shut proximity of the ureter and the perimeter of the cervix between the uterine artery and the vaginal fornices-a distance that usually is about 1 cm. During laparoscopic hysterectomy, care is taken to lateralize the pedicle containing the uterine vessels and subsequently use the uterine manipulator to elevate the lateral fornices, thereby rising the gap between the colpotomy and the ureter. The ureter can be protected by decreasing the chance of thermal injury related to energy-based dissection and vessel sealing. The microprocessor-based gadgets had been initially developed for laparoscopic surgical procedure, but, increasingly, these systems are being adopted for each laparotomic and vaginal use. Critical to safe use is each consciousness of the diploma of lateral thermal spread associated with the device in use and clarity concerning the situation of the ureters in the operative subject. Furthermore, and notably with ultrasonic devices, "retained warmth" within the oscillating jaw may be such that, for so much of seconds following deactivation, the device is able to inflicting thermal coagulation. Recognition Urologic injuries may be advised or identified intraoperatively by direct visualization of both damage or leakage of urine within the pelvis, or by way of intraoperative cystoscopy. If the harm is missed, and particularly when there exists a thermal damage, the analysis might not happen until later within the postoperative part of care. Bladder harm may be acknowledged intraoperatively by direct visualization, the presence of hematuria, and/ or particularly during laparoscopy, by the appearance of pneumaturia (air in the Foley catheter system). When suspected, the bladder could additionally be backfilled with an appropriate dye answer, as described above, to localize the defect by way of extravasation into the peritoneal cavity. Cystoscopy can be carried out to examine the bladder endothelium for trauma or defects.
Cheap 2.5 mg altace with visaTularemia Tularemia is brought on by Francisella tularensis blood pressure medication and weight loss 5 mg altace discount visa, a gram-negative coccobacillary organism that infects small mammals and is transmitted to people by insect vectors arrhythmia beta blockers cheap altace 5 mg overnight delivery. Although a number of totally different forms of medical presentation could happen with tularemia, relying on the mechanism of transmission and the location of entry, pulmonary tularemia secondary to inhalation of F. Inhalational anthrax characteristically produces a widened mediastinum on chest radiograph. Chest radiography shows patchy consolidation which may be accompanied by hilar lymphadenopathy and pleural effusions. Corticosteroid remedy for sufferers hospitalized with community-acquiredpneumonia:asystematicreviewandmeta-analysis. Atypical pneumonia: updates on Legionella, Chlamydophila, and Mycoplasmapneumonia. Index case of fatal inhalational anthrax due to bioterrorism within the United States. At the flip of the twentieth century, tuberculosis was the one commonest explanation for death in the United States; greater than 80% of the inhabitants was contaminated before the age of 20 years. At the beginning of the twenty first century, tuberculosis supplied a stark instance of the disparity in health resources between industrialized nations and the growing world. In the United States and Europe, few diseases have declined so greatly in frequency of instances and mortality as tuberculosis. Two major elements have been responsible: general improvement in living circumstances and the development of effective antituberculous chemotherapy, which has made tuberculosis a curable disease. However, in international locations with fewer sources, the disease continues to be a health crisis, typically hanging the younger, most efficient, members of society. Despite this big burden of disease, the variety of global deaths fell 22% between 2000 and 2015 because of the increased availability of diagnostic techniques and medications. The overwhelming majority of cases of lively tuberculosis happen in growing countries. This article evaluations the pathophysiology and scientific manifestations of tuberculosis, in addition to diagnosis and management. The epidemiology, prognosis, and therapy of disease attributable to nontuberculous mycobacteria are additionally reviewed. Keywords Tuberculosis Latent tuberculosis Tuberculosis, pulmonary Tuberculosis, miliary Mycobacterium tuberculosis Tuberculosis, multidrug-resistant Extensively drug-resistant tuberculosis Nontuberculous mycobacteria Mycobacterium infections, nontuberculous Tuberculosis and Nontuberculous Mycobacteria n 315 of tuberculosis combined to lead to an increasing frequency of instances. Fortunately, since 1991, the variety of instances reported yearly in the United States has once more been lowering. Perhaps most alarming is the comparatively current emergence of drugresistant strains of the organism, some of that are proof against a quantity of antituberculous drugs. The World Health Organization estimated roughly 480,000 new cases of multidrug-resistant tuberculosis worldwide in 2015, practically half of which were from India, China, and Russia. An important property of the tubercle bacillus is its capacity to retain sure stains even after exposure to acid (discussed beneath Diagnostic Approach); thus mycobacteria are said to be acid-fast. Transmission of the illness occurs via small aerosol droplets, usually from 1 to 5 �m in dimension, that comprise the microorganism. The source of these droplets is a person with tuberculosis who harbors the organism, typically excreting tubercle bacilli in the sputum or in small droplets produced throughout commonplace actions corresponding to talking, coughing, singing, and laughing. Most generally, transmission occurs with comparatively shut contact, typically between related individuals or others living in the identical household. When droplets containing mycobacteria are inhaled and reach the alveoli, a small focus of main infection develops, consisting of the organisms and an inflammatory process mounted by the host. After the initial an infection has began, organisms frequently spread through lymphatic vessels to draining hilar lymph nodes in addition to by way of the bloodstream to distant organs and other regions of the lung, particularly the apices. This sensitization and growth of a cell-mediated immune response usually happen within a number of weeks of initial publicity. The patient normally is unaware of the primary an infection, though a mild, self-limited febrile sickness could also be reported. In a small minority of sufferers, in all probability 5% or fewer, protection mechanisms are unable to control the primary infection, and clinically obvious major tuberculosis outcomes. Even when the first an infection apparently has been controlled, the tubercle bacillus will not be fully eradicated from the host. A small variety of organisms often remain in a dormant or latent state, not proliferating or inflicting any obvious active disease, however still potentially viable. However, in some patients, the delicate balance between the organism and the host protection mechanisms ultimately breaks down, typically after a few years, and a dormant focus of infection Transmission of tuberculosis is by inhalation of small aerosol droplets containing the organism. Such sufferers with active disease occurring at a time removed from the primary an infection are stated to have reactivation tuberculosis. For each main and reactivation disease, the lungs are essentially the most commonly affected website. However, with both type of disease, distant organ systems may be involved as a outcome of hematogenous spread in the course of the major phase of the an infection. In addition, disseminated disease known as miliary tuberculosis could outcome from the hematogenous spread of the organisms. The danger of developing energetic tuberculosis is best inside the first 2 years after the preliminary infection; about one-half of patients who develop lively illness do so inside this time frame. Tuberculous illness (or lively tuberculosis), however, is defined by the presence of clinically active disease in one or more organ systems, ideally with confirmation of the analysis by isolation of M. Other phrases price defining are those that describe totally different subsets of tuberculous disease. Most frequent are the phrases major and reactivation tuberculosis, which refer to illness following the preliminary exposure and illness that reactivates after a interval of latency, respectively. Several other terms are typically used to describe clinical disease on the premise of the presumed pathogenesis. The term progressive main tuberculosis reflects primary disease that has not been managed by host protection mechanisms and has continued to be energetic beyond the purpose at which delayed hypersensitivity has developed. As a basic rule, mobile immunity develops 2 to 10 weeks after the initial infection, and continuing energetic illness past this time has most of the features of reactivation tuberculosis. The time period postprimary tuberculosis refers to illness beyond the preliminary main an infection. Although this time period often refers to reactivation illness, it generally includes cases of progressive primary tuberculosis. The time period reinfection tuberculosis refers to illness in a beforehand infected person who outcomes not from reactivation of dormant tubercle bacilli however from new exposure to one other source of organisms. It is believed that people with prior publicity to tuberculosis who manifest delayed hypersensitivity to the organism are comparatively proof against exogenous reinfection from another source. The main infection in the lung consists of the organisms and a relatively nonspecific inflammatory response in the concerned region of parenchyma. Regional lymph nodes typically turn into involved by local unfold of the organism, and the combination of the first area in the lung (the Ghon lesion) and involved lymph nodes is termed a Ghon complex. When delayed hypersensitivity is present, either weeks after the primary an infection or during a period of reactivation disease, a unique pathologic pattern emerges. The hallmarks are the presence of (1) granulomas (collections of activated blood- and tissue-derived macrophages termed epithelioid histiocytes surrounded by a rim of lymphocytes), and (2) caseous necrosis (foci of necrosis and softening at the heart of a granuloma).
Effective 2.5 mg altaceChest wall compliance further decreases with age hypertension drug list 2.5 mg altace best, and respiratory complications of uncorrected kyphoscoliosis turn out to be more and more prevalent as the patient grows older causes 0f hypertension purchase altace 2.5 mg with visa. Marked distortion of the chest wall causes underventilation of some regions of the lung, microatelectasis, ventilation-perfusion mismatch, and hypoxemia. Disorders of the Respiratory Pump n 255 frequent causes of hypoxemia in kyphoscoliosis are hypoventilation and ventilationperfusion mismatch. A frequent complication of extreme kyphoscoliosis is pulmonary hypertension and cor pulmonale. Hypoxemia is an important trigger for the event of pulmonary hypertension. However, increased resistance of the pulmonary vessels additionally outcomes from compression and probably from impaired growth in areas where the chest wall is very distorted. Long-standing hypoxemia and pulmonary hypertension finally result in remodeling of the pulmonary vasculature, and the pulmonary hypertension turns into irreversible, even with correction of hypoxemia. Exertional dyspnea is probably the most common symptom skilled by patients with extreme kyphoscoliosis and respiratory impairment. Severe instances of kyphoscoliosis are usually characterized by hypercapnia and hypoxemia. The latter normally is because of each hypoventilation and ventilation-perfusion mismatch. Chronic respiratory insufficiency and cor pulmonale are the top outcomes of severe kyphoscoliosis, and the level of respiratory problem appears to correlate with the severity of chest wall deformity. Surgical therapy aimed toward bettering or correcting the spinal deformity could also be useful in children or adolescents but rarely is effective in adults. Supportive remedy that might be useful includes quite so much of measures that provide ventilatory help to the patient. Treatments with an intermittent positive-pressure respiratory machine increase tidal quantity by delivering positive strain to the patient during inspiration. The increase in tidal quantity improves microatelectasis and lung compliance, affording the affected person several hours with decreased work of breathing after every treatment. At evening, ventilatory help with inspiratory optimistic pressure delivered via a masks or via a tracheostomy tube allows the respiratory muscles to relaxation. Nocturnal ventilatory assist might present sufficient rest for the inspiratory muscle tissue to diminish daytime respiratory muscle fatigue. Obesity Obesity has many consequences for health, and respiratory signs are one facet. Obesity can produce a large spectrum in severity of respiratory impairment, starting from no signs to marked limitation in perform. This is partially defined by the distribution of physique fat: central (abdominal) distribution of fats is more related to decreased lung perform as measured by pulmonary perform testing. A full clarification of the discrepancies in symptoms amongst different patients is based on several factors, including smoking historical past, underlying lung disease, results of weight problems on the cardiovascular system, and underlying physical deconditioning. Restrictive sample on pulmonary operate exams 256 n Principles of Pulmonary Medicine Features of obesity are: 1. Specifically, Joe had options of large weight problems, hypersomnolence, and peripheral edema, the latter presumably associated to cor pulmonale and right ventricular failure. With the accumulation of knowledge about the pathogenesis of respiratory impairment in obesity, the time period pickwickian syndrome has turn into much less meaningful. As a results of extra soft tissue, extra work is important for enlargement of the thorax. In addition, the huge accumulation of soppy tissue within the stomach wall exerts strain on abdominal contents, forcing the diaphragm as a lot as a higher resting position. The excessive resting position of the diaphragm in obesity, occurring as a outcome of strain from the obese abdomen, is associated with decreased expansion of the lung and closure of small airways and alveoli at the bases. Thus the dependent regions are hypoventilated relative to their perfusion, and this ventilation-perfusion mismatch contributes to arterial hypoxemia. In a fashion much like that of kyphoscoliosis, weight problems results in lower tidal volumes and elevated wasted or lifeless space ventilation. To maintain enough alveolar air flow, general minute air flow must enhance in the face of elevated work of respiration. Most patients compensate appropriately by growing their total minute ventilation, and Pco2 stays regular. Most overweight sufferers have increased central respiratory drive in response to the added mechanical load. This appears to be an acquired phenomenon and may develop due to sleep-disordered respiratory. Another distinguishing feature between normocapnic and hypercapnic overweight patients may relate to inspiratory muscle power. Another issue that contributes to the general clinical picture in lots of massively obese sufferers is higher airway obstruction during sleep. Soft tissue deposition in the neck and tissues surrounding the higher airway presumably predisposes the individual to episodes of full higher airway obstruction during sleep (see Chapter 18). Although weight problems, irregular respiratory drive, respiratory muscle weakness, and sleep apnea syndrome contribute to respiratory dysfunction, precisely how they work together in particular person sufferers is usually difficult to assess. The signs which will happen in obese patients can be associated with elevated work of breathing. Venn diagram reveals hypothetical indication of the best way obesity interacts with obstructive apnea and irregular respiratory drive. These issues are largely related to arterial hypoxemia both through the day and at night time, particularly if sufferers have sleep apnea syndrome. In most overweight sufferers, arterial blood gases present a lower in Po2 and an increase in AaDo2 as a consequence of excessive diaphragms, airway and alveolar closure, and ventilation-perfusion mismatch. If sufferers have sleep apnea syndrome, arterial blood fuel values become even more deranged at night throughout episodes of apnea. Weight loss is crucial within the treatment of overweight patients with respiratory dysfunction. If weight loss is efficiently achieved by either food plan or bariatric surgical procedure, respiratory problems could resolve in some sufferers. Nocturnal positive-pressure ventilation is generally helpful in bettering daytime sleepiness, particularly if the affected person has concomitant obstructive sleep apnea syndrome (see Chapter 18). In some patients who hypoventilate, respiratory stimulants, especially progesterone (a centrally performing respiratory stimulant), have been used with restricted success. Sleep-disordered breathing in neuromuscular disease: diagnostic and therapeutic challenges. Practical respiratory management in amyotrophic lateral sclerosis: evidence, controversies and up to date advances.
Buy altace 2.5 mg with visaGoverned by the interplay between living tissue and ultrasound hypertension 10 cheap altace 2.5 mg fast delivery, slicing velocity is directly related to tissue traction and blade floor space arteria maxillaris altace 5 mg discount otc, and inversely to tissue elasticity. The quickest cutting with the least amount of coagulation occurs when tissue is positioned on tension and firmly compressed, lifted, or rotated with the sharpest side of the blade (for instruments with completely different blade interfaces). On the other hand, maximum coagulation is best achieved by relaxing pressure and utilizing the blunt edge of the blade. Consequently, the surgeon should all the time be aware of the potential for untimely incision of a vascular pedicle from making use of an excessive quantity of pressure or traction before full desiccation. The most essential risk related to ultrasonic devices is their propensity to store warmth in the shaft and blade, which can remain above the 60�C threshold for fast cell death for lots of seconds following deactivation. The risk for inadvertent tissue damage may be lowered by ensuring adequate visualization during activation and taking care to avoid manipulation or contact with visceral tissues immediately after activation. For each these units, compression of the articulated jaw allows for chopping or sealing relying on the tour of the blade, the diploma of compression of tissue, and the quantity of "lift" applied by the surgeon. Science turns into art, and art turns into function when elementary rules are utilized to dictate surgical follow. Guided by the Hippocratic charge to "primum non nocere," the final word aim of energy-assisted surgery is the attainment of anatomical dissection and hemostasis with the least amount of collateral harm and subsequent scar tissue formation. Regardless of the chosen modality, the inseparable and exponentially linked elements of time and the quantity of delivered power must be built-in while purposefully moderating to attain the desired tissue impact. If the bowel, bladder, or ureter is in shut proximity to a bleeder, they should be sufficiently mobilized earlier than applying power. Thermal vitality should all the time be withheld till an orderly sequence of anatomical triage is carried out. Demonstration of the potential of ultrasonic shears to injure tissue after deactivation. Patient safety during laparoscopic monopolar electrosurgery: ideas and tips. Energy Systems in Laparoscopy: A Practical Manual of Laparoscopy and Minimally Invasive Gynecology. Insulation failure in robotic and laparoscopic instrumentation: a prospective analysis. Surgical problems particular to monopolar electrosurgical vitality: engineering adjustments which have made electrosurgery safer. The affected person with a cardiac pacemaker or implanted defibrillator and administration throughout anaesthesia. Electromagnetic interference brought on by widespread surgical energy-based devices on an implanted cardiac defibrillator. Factors affecting capacitive current diversion with a uterine resectoscope: an in vitro study. Mechanisms of thermal injury to the decrease genital tract with radiofrequency resectoscopic surgery. Residual warmth of laparoscopic vitality units: how lengthy should the surgeon wait to touch further tissue Troubleshooting gear issues is a vital step in surgical procedure and should be mastered by each laparoscopic surgeon. Each of those competencies shall be described intimately, referring, as appropriate, to different related chapters within the textual content. This decisionmaking course of requires integrating the patient targets with the surgical goals as well as careful consideration of potential obstacles to , and benefits of, given medical and surgical approaches to the problem. A thoughtful dialog should happen with the patient prior to surgical procedure designed to assess her expected consequence, and to affirm that such an consequence is realistically feasible. When contemplating laparoscopic surgery, a danger evaluation should be carried out evaluating the issue degree of the process and potential limitations to success. Two common obstacles encountered in laparoscopic surgery are intra-abdominal adhesions (from earlier surgery, infection, or endometriosis) and the scale of pathology (uterine or adnexal). A concerted effort should be made to anticipate these preoperatively and plan appropriately. A detailed history, physical exam, and, the place appropriate, imaging research, will alert the surgeon to the risk of adhesions or pelvic or abdominal lots. Review of earlier operative reports will help prepare for the upcoming procedure as nicely. It is quite a reflection of the entire course of of debate and counseling throughout which sufferers are knowledgeable of their analysis, the pure history of the dysfunction, and the total spectrum of options for treatment, together with "watchful ready," and forty seven forty eight Principles of laparoscopic surgery Table 4. Patient selection Patient preparation Operating room group Patient positioning Peritoneal entry Creation and imaging of the operative field Tissue and fluid manipulation Cutting and hemostasis Tissue approximation Specimen management and extraction Wound administration Postoperative care which will incorporate each medical and surgical management. Similarly, the surgeon ought to provide sensible expectations for surgical outcomes based on private experience and applicable medical literature. Occasionally, sudden pathology could also be found on the time of laparoscopic surgery. Examples include an sudden tumor, abnormal appendix, or identified or suspected pathology more severe than anticipated. Depending on surgeon talent and availability of sources such as different consultants, it could be potential to attempt to manage the unexpected discovering at the time of surgical procedure. In some cases, it could be prudent to terminate the process and revisit the plan and method with the patient sooner or later. The bioethical principle of nonmaleficence ("first, do no hurt") could also be utilized in most of these circumstances. When one can anticipate the presence of concomitant pathology corresponding to involvement of the appendix in extreme endometriosis, applicable consultation and consent ought to be obtained. In obese sufferers, working with a multi-disciplinary health-care staff, that could include a dietician and bodily therapist, could facilitate weight reduction previous to an elective procedure and attendant reduction in associated perioperative risks. A careful medical and surgical history should be reviewed with the affected person previous to surgical procedure. In such circumstances, routine laboratory investigations is in all probability not beneficial however, as a substitute, must be ordered as applicable primarily based on the scientific image. Expected postoperative restoration together with discussion of the anticipated time required to be away from work and activities of daily dwelling. In tutorial establishments, patients ought to be made aware of the position of trainees similar to college students, residents, and fellows in their surgery and perioperative care, in addition to using multimedia recording. For example, surgical administration of endometriosis can differ considerably relying on whether or not the goal is to enhance fertility or to cut back pelvic pain. If a particular surgical process is deemed outside their scope of apply, acceptable referral to surgical specialists should be made. Choice of assistant, nursing, and anesthesiologist is also essential to think about preoperatively. An assistant for vaginal or uterine manipulation can additionally be typically required for complex gynecologic procedures. Layout of the working room Laparoscopic surgical procedure requires the use of extremely specialized and technical gear; the surgeon is liable for understanding safe and efficient perform of these parts, together with, if essential, the assembly and troubleshooting of instrumentation.
|