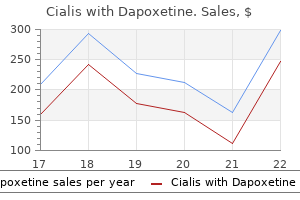
Cialis with dapoxetine 20/60mg discount with visaAwake surgery with continuous motor testing for resection of brain tumors within the major motor area erectile dysfunction protocol book review buy cheap cialis with dapoxetine 20/60 mg line. Anesthesia administration of awake craniotomy carried out beneath asleep-awake-asleep technique utilizing laryngeal mask airway: report of two cases erectile dysfunction pills viagra buy 20/60 mg cialis with dapoxetine mastercard. Maintenance of normotension or slight hypotension is necessary to reduce bleeding and brain swelling that can occur throughout brain publicity, and to achieve surgical hemostasis. Severe arterial hypertension and tachycardia are associated with a big risk of postoperative intracranial hemorrhage and myocardial ischemia, respectively, and ought to be prevented or promptly treated [20]. Several agents can be used to decrease blood strain, including beta blockers (esmolol, metoprolol, atenolol), calcium-channel blockers (diltiazem and verapamil), alpha blockers (urapidil) combined alpha and beta blockers (labetalol), and alpha-adrenergic receptor agonists (clonidine). Conclusion Awake craniotomy is a well-tolerated procedure that requires an intensive knowledge of underlying neuroanesthesia rules, as properly as specific strategies of local anesthetic scalp blockade, superior airway administration, a devoted sedation�analgesia protocol, and skillful management of systemic and cerebral hemodynamics. Recent developments in the anesthetic administration of craniotomy for supratentorial tumor resection. Awake insertion of the laryngeal mask airway utilizing topical lidocaine and intravenous remifentanil. The impact of scalp block and local infiltration on the haemodynamic and stress response to skull-pin placement for craniotomy. Combination of bupivacaine scalp circuit infiltration with basic anesthesia to control the hemodynamic response in craniotomy sufferers. Effect of a subanesthetic dose of intravenous ketamine and/or native anesthetic infiltration on hemodynamic responses to skull-pin placement: a prospective, placebo-controlled, randomized, double-blind study. Prevention and remedy of local anesthetics-induced complete atrioventricularblock throughout awake craniotomy. Transient facial nerve palsy after auriculotemporal nerve block in awake craniotomy sufferers. Training anesthesiology residents in providing anesthesia for awake craniotomy: learning curves and estimate of wanted case load. Rapid development of tolerance to analgesia throughout remifentanil infusion in humans. Management of hypertensive emergencies in acute mind illness: analysis of the therapy results of intravenous nicardipine on cerebral oxygenation. To higher achieve it, the modern anesthesiologist should use drugs with a predictable and favorable profile: a speedy onset and offset, protected and rapid induction, early recovery, easily titratable and with out - or minimal - adverse or negative effects. Pending the event of new and "almostideal" medication, the emergence and enchancment of methods and units that allow their protected and correct supply, have contributed to the event of our apply. Thus, the talk continues on intravenous and inhalation anesthesia regarding well-defined clinical endpoints. These are mainly related to the velocity and restoration of anesthesia, hemodynamic adjustments, operative situations, postoperative nausea and vomiting, recovery of psychomotor and cognitive operate, and discharge from hospital. Costa (*) Department of Anesthesiology, Centro Hospitalar Lisboa Central, Lisbon, Portugal e-mail: martinsdacosta. Lobo Department of Anesthesiology, Hospital Geral de Santo Ant�nio � Centro Hospitalar do Porto, Porto, Portugal � Springer International Publishing Switzerland 2017 Z. Furthermore, analysis on long-term outcomes has shown that intravenous anesthesia with propofol may be extra favorable concerning cancer recurrence after surgery [3]. Although several contradictory results have been published regarding immunosuppression, plainly propofol attenuates surgical stress response with out impairment of natural killer cell activity and leading to less important immunosuppression [4]. Aware of the advantages described, economic influence has been a topic of nice interest with inadequate research till now. Therefore, all costs and benefits must be thought of, associated not only to the technique but in addition the institution, the affected person, and the society [5]. Nevertheless, we should not neglect the safety and simple titration of volatile anesthetics and acknowledge the deserves of each strategies [6]. Clear indications for using every method are lacking and the selection seems to be more related to the individual expertise and familiarity with the technique than based mostly on published research, without forgetting the supply of the equipment. The follow of target-controlled anesthesia is based on fundamental pharmacokinetic and pharmacodynamic concepts which deserve an in depth review. Drug elimination by metabolism from the central compartment corresponds to the fixed K10. They are the- oretical volumes that can be remotely thought because the blood volume (V1), a "vessel wealthy" compartment (V2) and a "vessel poor" compartment (V3). In every model, the dimensions of the volumes of distribution displays the solubility of the drug in that particular compartment. For pharmacokinetic/pharmacodynamic modeling, an effect-site compartment may be added. Due to its negligible quantity, the rate constants for motion in and out of this compartment are the identical (K1e = Keo). In the past a long time, pharmacokinetic fashions have been developed and improved, allowing better understanding of the behavior of various medication and making attainable the adjustment to the individual kinetics. It is defined because the focus at regular state multiplied by the clearance worth (Cl). Generally, it can be calculated knowing the dose present in the physique (D) and its plasma focus (C): Vd = D / C (13. Half Life (t1/2) is the time taken for the concentration of a drug to drop by half its value. However, since most medicine are distributed in a couple of compartment and clearance from each occurs at different charges, the drug could have multiple t1/2. Decremental time is a similar idea that defines the time required for blood concentration to decrease to a desired percentage. Both ideas are helpful predictors of drug concentration decline after an infusion is stopped. If one other bolus is required to increase the goal focus, New Loading Dose = (Cf - Ci) � Vd; (13. Clearance (Cl) describes the volume during which the drug is eliminated during a unit of time (mL/ min or mL/hr). For this cause it becomes obvious that the main impact is delayed in addition to the drug concentration at the impact web site when in comparability with the plasma peak concentration. Hysteresis represents this time delay between plasma compartment and effect-site compartment. Mathematically, the time taken for blood�effect-site equilibration is described by the rate fixed Ke0 which is totally different for various medication. T1/2 Ke0 is the time taken for the drug concentration in the effect web site to attain half of the concentration in the blood and could be clinically extra useful than Ke0. The computer system with its mathematical algorithm calculates the specific parameters for each affected person, as Vd and Cl.
Generic 20/60mg cialis with dapoxetine otcElderly sufferers [61] who received massive volume resuscitation with marginal cardiac operate are at vital threat of pulmonary edema 48�96 h postoperatively erectile dysfunction stress discount cialis with dapoxetine 40/60mg overnight delivery. Signs of impending respiratory failure embrace Most patients with spinal twine harm would require care and frequent monitoring within the intensive care unit initially erectile dysfunction drugs causing buy cialis with dapoxetine 20/60 mg with amex. Patients typically current with hypotension due to the decreased peripheral vascular resistance. Occasionally, sufferers can present with hypovolemic shock due to blood loss in addition to neurogenic shock. Souter progressive hypercapnea, and/or hypoxemia, declining compelled very important capacity or unfavorable inspiratory stress, and increased speedy shallow respiration index (low tidal volume and elevated respiratory rate). In addition, power of the respiratory muscle tissue must be assessed every day by measuring most unfavorable inspiratory pressure and compelled important capacity [57]. Patients with high cervical spine injury are vulnerable to a phenomenon generally known as "ping-pong" atelectasis, and seem to respond properly to higher tidal volumes. Consequently, once the affected person is not in danger for lung harm, our method is to liberalize the tidal quantity progressively to 12�15 ml/ kg of perfect physique weight [64]. Early tracheotomy could additionally be indicated in sufferers with high cervical spine damage with no expectation of recovery of sufficient spontaneous air flow [65, 66]. This procedure can help in secretion clearance and permit for decreased level of sedatives and analgesics, as a tracheotomy appears to be higher tolerated than an endotracheal tube [65]. Alternatively, if the affected person fails to wean from the mechanical ventilator for different reasons, a tracheotomy ought to be thought-about within 10�14 days from day of admission [67, 68]. The interventions embrace respiration workouts, bronchodilator treatment, and mechanical cough assist. For secretion clearance, sufferers endure cough assist by way of a mechanical insufflator�exsufflator several instances a day, and chest physiotherapy if a focal consolidation is recognized on chest radiograph [57]. They are often given scheduled ipratropium or tiotropium for bronchospasm prevention [69]. Low molecular weight heparin is the popular anticoagulant of selection [72, 73] but a mixture of unfractionated heparin with sequential compression gadget seems to be equally effective [74]. Frequent turning (every 2�3 h) and heel elevation utilizing specialized foam boots are effective in stopping ulcer formation [80]. Generally, trauma patients are hypermetabolic and require dietary help for wound healing. In addition, early feeding can improve gastric mucosa blood flow and will stop stress ulceration. Review of the secondary injury concept of acute spinal wire trauma with emphasis on vascular mechanisms. Secondary damage mechanisms of spinal wire trauma: a novel therapeutic method for the administration of secondary pathophysiology with the sodium channel blocker riluzole. The role of excitotoxicity in secondary mechanisms of spinal twine damage: a evaluate with an emphasis on the implications for white matter degeneration. Treatment of spinal cord injury with intravenous immunoglobulin G: preliminary proof and future perspectives. An aggressive bowel regimen together with daily digital stimulation should be used to avoid stool impaction, which may within the quadriplegic induce a respiratory embarrassment that transcends "easy constipation. Early mobility with occupational and physical therapy is essential in limiting contracture formation. Patients and families may also benefit from additional counseling by a rehabilitation psychologist, as grief reactions can often be extended and extreme. As the protection of motor vehicles and the quality of prehospital enhance, more individuals are surviving the preliminary trauma. The global map for traumatic spinal wire injury epidemiology: update 2011, global incidence price. Brown-S�quard syndrome after a gun shot wound to the cervical backbone: a case report. Administration of methylprednisolone for 24 or forty eight hours or tirilazad mesylate for 48 hours within the remedy of acute spinal wire harm. Results of the third nationwide acute spinal cord harm randomized controlled trial. Beneficial effect of methylprednisolone sodium succinate in the remedy of acute spinal wire harm. Methylprednisolone in the administration of spinal cord injuries: classes from randomized, controlled trials. Dynamic adjustments in arterial waveform derived variables and fluid responsiveness in mechanically ventilated patients: a systematic evaluate of the literature. Abilities of pulse strain variations and stroke quantity variations to predict fluid responsiveness in prone place throughout scoliosis surgical procedure. A systematic evaluate of the prevalence of musculoskeletal pain, again and low again pain in individuals with spinal wire damage. Electrocardiographic abnormalities in the early stage following traumatic spinal twine damage. Cardiovascular penalties of lack of supraspinal management of the sympathetic nervous system 6 Spinal Cord Injury after spinal wire damage. Influence of neurological lesion level on coronary heart price variability and fatigue in adults with spinal wire harm. Predictors of hospital mortality and mechanical ventilation in patients with cervical spinal cord injury. Time-courses of lung perform and respiratory muscle strain generating capability after spinal cord damage: a prospective cohort examine. Specialized respiratory management for acute cervical spinal twine injury: a retrospective analysis. The effectiveness of early tracheostomy (within at least 10 Days) in cervical spinal twine injury patients. Abdominal binder improves lung volumes and voice in people with tetraplegic spinal cord damage. Roussi J, Bentolila S, Boudaoud L, Casadevall N, Vall�e C, Carlier R, Lortat-Jacob S, Dizien O, Bussel B. Contribution of D-Dimer determination within the exclusion of deep venous thrombosis in spinal twine injury sufferers. Thromboprophylaxis in sufferers with acute spinal injuries: an evidence-based evaluation. Hospital-acquired stress ulcers in spinal twine injured patients: time to occur, time until closure and risk components. Prevention of pressure ulcers among individuals with spinal wire harm: a systematic evaluate.
Cialis with dapoxetine 40/60 mg discount mastercardMaximum systolic velocity must be measured utilizing multiple views erectile dysfunction pumps side effects cialis with dapoxetine 40/60mg buy generic on line, a time scale on the xaxis of a hundred mm/s erectile dysfunction meds online cialis with dapoxetine 20/60mg purchase with mastercard, and a grey scale that allows visual separation of noise from the true velocity sign. Also the effects of stress recovery, the conversion of kinetic vitality into potential vitality with a corresponding enhance in pressure distal to a stenosis, are ignored, however these are usually small until aortic diameter is <3 cm. Maximum velocity and imply strain gradients across a stenotic aortic valve are each flow dependent. Despite these limitations, continuity equation valve area calculations have been properly validated [2,3]. Likewise, the peak Dopplerderived gradient by echo correlates properly with the height instantaneous transvalvular gradient at cardiac catheterization (although this is rarely calculated or reported). Increased wall thickness causes the left ventricle to become stiffer and fewer compliant and thus higher enddiastolic pressures are required to maintain left ventricular filling. This, in turn, results in larger left atrial pressures and elevated pulmonary capillary wedge pressures. In the catheterization laboratory, the calculation of aortic valve space is traditionally performed using the Gorlin formulation. This formulation was initially derived within the early 1950s in patients with mitral stenosis. Although the Gorlin formula is seemingly simple, there are a variety of potential pitfalls and meticulous element is critical to acquire an correct estimation of aortic valve space. The Gorlin formula requires measurement of cardiac output, coronary heart fee, systolic ejection interval, and mean transvalvular gradient. Aortic stenosis 111 output may be obtained either by thermodilution or by way of the Fick method. This demonstrates that the pressure gradient is primarily because of an obstruction between the ascending aorta and right femoral artery. Potential pitfalls in utilizing femoral artery stress to measure aortic valve gradient could be remedied by utilizing either a pressure wire or a double lumen pigtail, thus permitting simultaneous measurement of left ventricular and central aortic valve pressure. Careful consideration to detail and examination of the fidelity of the left ventricular waveform are crucial. In basic, catheter pullback throughout the aortic valve is a suboptimal approach to measure aortic valve gradients. The reason for the stress gradient on this patient was an obstruction in the femoral artery sheath that was dislodged with manipulation of the catheter. The problem lies in the numerator of the Gorlin equation; particularly, the correct willpower of flow throughout the aortic valve. Examination reveals a blood stress of 136/80 mm Hg and a delayed carotid upstroke. There is a late peaking systolic ejection sort murmur heard finest on the right upper sternal border radiating to the carotids. Doppler evaluation demonstrated an aortic velocity of 4 m/s similar to a peak instantaneous gradient of sixty four mm Hg and a imply gradient of 50 mm Hg. Note the massive mean transvalvular gradient of one hundred ten mm Hg and slow upstroke of the aortic tracing. This phenomenon happens within the setting of a extremely stenosed valve, because the extra occlusive effect of the catheter throughout the valve is sufficient to additional decrease aortic strain. Dynamic subvalvular stenosis is primarily due to hypertrophic cardiomyopathy (reviewed in Chapter 15). Accurate evaluation of aortic stenosis: a evaluate of diagnostic modalities and hemodynamics. Modification of the simplified formulation for mitral and aortic valve area calculation. In particular, pure aortic valve insufficiency, bicuspid aortic valves, and disrupted aortic valves from ascending aortic aneurysms or dissections are greatest handled surgically, albeit with some exceptions. Because the transvalvular aortic strain gradient is dependent on flow throughout the valve squared, a low move state. Echocardiographic evaluation reveals poor aortic valve leaflet mobility, which is primarily due to the myocardial disease and low circulate state quite than inherent calcific aortic pathology. A dobutamine challenge can additionally be helpful in order to assess for contractility and/ or circulate reserve. Contractile reserve has important prognostic implications, since its absence portends a poor prognosis regardless of valve replacement. Invasive hemodynamics are an integral part of periprocedural affected person monitoring as they help establish potential complications that will occur. Noting this at the start of the procedure is useful, because a big reduction in diastolic blood pressure following valve deployment is usually a signal of severe aortic valve insufficiency and/or paravalvular leak. The excessive transvalvular strain gradient and delayed aortic stress upstroke confirm the prognosis. Hypotension could point out ventricular perforation with cardiac tamponade, extreme mitral valve regurgitation because of catheter or wire entanglement into the mitral valve cords and leaflets, or critical vascular harm, normally on the website of vascular entry. A pulmonary artery catheter and transesophageal echo, if available, can help shortly differentiate among these potential issues. Severe mitral regurgitation usually ends in a large V wave on wedge tracing, while cardiac tamponade is related to an elevated central venous strain and equalization of diastolic pressures. Vascular trauma and hemorrhagic shock normally manifest with a low central venous strain (Table 9. Although selfexpanding transcatheter valves may be deployed at lower pacing rates of 90�100 bpm, the concept of diminishing cardiac output stays paramount. The aortic systolic pressure should lower beneath 50 mm Hg before inflating the aortic valvuloplasty balloon. A low diastolic aortic stress with a wide pulse stress may be the first indication of severe aortic valve insuffi ciency. These sewing rings decrease the overall residual orifice area at the degree of the annulus. Additionally, the valve sizing is carried out prior to the process, which decreases the danger of undersizing the valve prosthesis. Transcatheter and surgical aortic valve alternative 127 Contemporary data out to 5 years and longer present secure hemodynamics of transcatheter valves [10,13]. After noting no surgical problems, this surveillance could additionally be prolonged to echocardiographic evaluations at 1�3year intervals. Cardiac catheterization with crossing of the valve for measurement of pressure gradients must be reserved just for interrogating a failing valve or when echocardiography is unable adequately to diagnose a suspected valvular concern. Severe aortic stenosis with low transvalvular gradient and severe left ventricular dysfunction: result of aortic valve substitute in 52 patients. Paradoxical lowflow, lowgradient severe aortic stenosis regardless of preserved ejection fraction is associated with greater afterload and lowered survival. Changes in arterial pressure throughout left coronary heart pullback in sufferers with aortic stenosis: an indication of extreme aortic stenosis. Aortic regurgitation index defines severity of periprosthetic regurgitation and predicts outcome in sufferers after transcatheter aortic valve implantation. Prosthetic coronary heart valves: selection of the optimum prosthesis and longterm management.
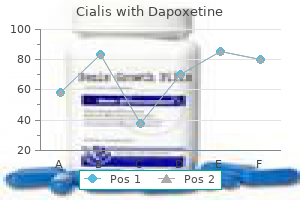
| Comparative prices of Cialis with Dapoxetine | | # | Retailer | Average price | | 1 | Whole Foods Markets | 564 | | 2 | ShopKo Stores | 511 | | 3 | DineEquity | 425 | | 4 | Army Air Force Exchange | 523 | | 5 | McDonald's | 980 | | 6 | Hy-Vee | 828 | | 7 | Limited Brands | 417 |
Cialis with dapoxetine 40/60 mg order on-lineOften a femoral head pusher can be used by the surgeon to facilitate discount by pushing the femoral head down into the acetabulum erectile dysfunction new zealand cialis with dapoxetine 40/60mg generic with amex. Specifically impotence yahoo discount cialis with dapoxetine 40/60mg with amex, posterior stability is assessed with flexion, adduction, and inside rotation of the hip until the femoral head begins to sublux out. Anterior stability is set by hip extension, external rotation, and adduction. Longitudinal traction can be pulled via the hip to assess gentle tissue pressure or shuck. Sometimes a bone hook on the neck trunnion is important to generate adequate traction to dislocate the hip. However, one should be careful to not torque the hip an extreme quantity of as a result of this will trigger a periprosthetic fracture. The cement should neither be too runny (which might result in blood laminations in cement and weakened mechanical strength) nor too doughy (preventing interdigitation into cancellous bone). Insert the stem on its deal with and hold in appropriate version whereas the cement hardens. Close the abductor tendon and vastus lateralis fascia with one nonabsorbable, braided suture in figure-of-8 fashion. There are typically no specific vary of movement or weight-bearing precautions for an anterolateral method and cemented hemiarthroplasty, which is why the authors prefer this mode of fixation and surgical approach. This cohort is usually frail and elderly, probably with cognitive decline, which makes compliance with any kind of restrictions difficult. Although the goal of physical remedy is to get the affected person again to the preinjury degree of ambulation and performance, ample literature suggests that the functional stage will decline to some extent. Postoperative radiographs are often obtained in the recovery room, including a low anteroposterior pelvis and a frog leg lateral of the affected hip. These are scrutinized for restoration of anatomy (offset/leg length and stem place and cement mantle). The authors use the approach described by Barrack and colleagues to assess cement mantle. Postoperative ache control is managed with a choice for oral medications and conservative use of narcotics given the propensity of this cohort for delirium and confusion and associated falls. Improved cementing techniques and femoral part loosening in younger patients with hip arthroplasty. Cemented versus uncemented hemiarthroplasty for displaced femoral neck fractures: a potential randomized trial with early follow-up. Cemented versus uncemented hemiarthroplasty for displaced femoral neck fractures: 5-year followup of a randomized trial. Displaced femoral neck fractures within the aged: hemiarthroplasty versus whole hip arthroplasty. Caesarean supply can currently be considered because the operation women the world over are more than likely to endure. Regardless of the type of entry, the surgical technique must comply with certain fundamental necessities. It must adequately expose the uterus, enable the fetus to be easily accessed and extracted, cut back the chance of postsurgical issues, and permit for an aesthetically pleasing result. There are two forms of cutaneous incisions: transverse (Pfannenstiel, Maylard, Cherney, Joel-Cohen) and longitudinal (median or paramedian). Most cesarean deliveries are carried out with a transverse incision of the skin and the muscle fascia using a way launched by Pfannenstiel in 1900 [1]. The transverse cutaneous incisions within the Pfannenstiel laparotomy are obviously performed in the same area, but along totally different strains close to the realm. Generally, all Pfannenstiel transverse incisions throughout cesarean delivery are carried out within the Malgaigne triangle space. The separation is completed by detaching with fingers or with the help of a wad of gauze on forceps. The rectus muscles are separated alongside the median line up to the base of the pyramidal muscles that are sectioned sagitally within the point of union, with out detaching them from the ipsilateral rectus muscle. The transversalis fascia and the peritoneum are cut vertically, being careful to keep away from the bladder. In fact when the bladder is empty, the bottom is approximately on the stage of the higher margin of the pubic symphysis. Locating the house of Retzius, especially throughout a repeated cesarean supply, prevents injury to the dome of the bladder. This virtual space is positioned in front of the exterior facet of the parietal peritoneum. It is above the bladder and characterised by lax cellular tissue which could be simply indifferent by finger fracture. In addition to aesthetic reasons, the transverse incision has numerous advantages that change depending on the direction and location of the opening of the stomach. It is the incision that finest adapts to the various stomach wall buildings and subsequently is able to facilitate the mending of broken tissues. Anatomical and practical damage is considerably less than that ensuing from longitudinal sections and may be repaired without compromising resistance of the fascia, which is actually an important construction by method of postoperative dehiscence. In truth, in longitudinal incisions the frequency of laparotomy wound dehiscence is eight occasions higher [2]. It is unsure whether or not this surgical approach can be useful when it comes to instant postoperative complications: Wall and colleagues have noticed in the vertical incision, in 239 overweight patients, a larger incidence of parietal complications, versus the transverse incision [3]. However, the postoperative course is improved, because the transverse incisions are frequently less painful. Cutaneous adhesion is extra rapid and solid, partly as a outcome of the lesser frequency of septic issues [3]. The restricted visibility may be improved by making sufficient use of the cutaneous incision and separating, vertically and laterally, the rectus muscle tissue from their sheath. The difficulties in extracting the fetus in the Pfannenstiel incision, when the size of the cutaneous supply is a minimal of 15 cm, are actually minimal and statistically comparable to the Mackenrodt�Maylard method [5]. This, however, remains restricted because it involves the larger branches of the exterior pudendal and superficial inferior epigastric arteries. For this purpose some authors imagine it must be contraindicated in case of coagulopathy or preeclampsia. The Mackenrodt�Maylard laparotomy, described in 1901�1907, includes the incision of the pores and skin and of the subcutaneous tissue from one anterior superior iliac backbone to the opposite, following a slight upward concavity. After the fascia is cut transversely, the rectus muscular tissues are separated, for a brief size, along the median line and are then isolated beneath the muscle venter as much as the lateral margin of the muscular tissues. This stage reveals the underlying decrease epigastric vessels which some authors would rather tie and ship to reduce blood loss. The rectus muscle tissue are then minimize transversely with scissors or electrical scalpel, ranging from the medial margin.
Cialis with dapoxetine 40/60 mg generic overnight deliveryA prolonged I-D interval leads to greater fetal exposure to nitrous oxide and the unstable halogenated agent lovastatin causes erectile dysfunction generic 40/60mg cialis with dapoxetine free shipping. Thus erectile dysfunction lifestyle changes cialis with dapoxetine 40/60 mg purchase overnight delivery, a chronic I-D interval could end in a higher threat of neonatal depression at delivery, regardless of the presence of regular umbilical twine blood gasoline and acid�base measurements [53,54]. The next section of this chapter reviews issues of common anesthesia in obstetrics, which are included in Box 18. Awareness during anesthesia the risk of maternal consciousness is the best between induction of general anesthesia and supply of the toddler. Administration of 50% nitrous oxide in oxygen without one other agent leads to maternal awareness in 12%�26% of cases [12,45]. Awareness is inhumane for the mom and leads to excessive maternal concentrations of catecholamines, which result in uterine artery vasoconstriction and lowered oxygen delivery to the fetus [55�64]. A frequent method to forestall consciousness is to administer 50% nitrous oxide in oxygen together with a low concentration of a volatile halogenated agent. This method is straightforward and reduces the incidence of maternal consciousness to lower than 1%. A low focus of a unstable halogenated agent is enough for most patients as a result of being pregnant decreases anesthetic necessities by as a lot as 30%� 40%. In most cases, we administer 30%�50% nitrous oxide in oxygen and a low concentration (0. Intraoperative consciousness can happen in emergent cesarean deliveries underneath common anesthesia in hemodynamically unstable sufferers unable to tolerate a enough depth of anesthesia. Intraoperative consciousness under general anesthesia might cause extreme postoperative psychological sequelae, including post-traumatic stress dysfunction, nervousness, neurosis, nightmares, worry of hospitals, and even demise [58]. Although 50% oxygen concentration is often required before supply, it has been proven that 33% of oxygen could be an appropriate various with out fetal compromise [59]. The B-Aware trial showed an 82% discount within the incidence of consciousness in sufferers susceptible to perioperative awareness including cesarean supply patients [63]. Difficult airway It is a common consensus that intubation of a full-term pregnant ladies could be tough for numerous causes, including non-pregnancy-related. The authors reported the incidence of adverse intubation in pregnant ladies to be as high as 1 in 20�30 (3. In another research failed intubation in pregnant ladies was reported to be 1 in 100�1316 (0. Difficult and/or failed intubation in obstetric population is known to be 8�10 occasions greater than that within the nonobstetric surgical inhabitants [6]. Two studies have reported fast and vital modifications (increase) in the Mallampati score throughout being pregnant and in labor [8,9]. In obstetric population, Mallampati classes three and four are strongly associated with troublesome laryngoscopy, with an elevated relative threat of seven. Kuczkowski and Benumof reported on the parturient with prepregnancy subglottic tracheal stenosis, which worsened during pregnancy, creating critical airway management dilemma [67]. The supraglottic airway gadgets have been used successfully in slim, fasted pregnant ladies for elective cesarean deliveries beneath basic anesthesia [24,25], in addition to rescue units for emergent troublesome airway administration [7]. With failed intubation and difficult masks air flow, the ProSeal may be most popular as it has a drain tube for the regurgitant fluid. The anesthesiologist (and the patient) must be prepared for common anesthesia in case of failed spinal anesthesia, whole spinal, cardiac arrest, large hemorrhage. A new technological development that may assist in instances of sudden troublesome intubation is videolaryngoscopy. If oxygenation satisfactory and steady, maintain oxygenation and begin cesarean delivery- ship child c. If air flow fails, or some other complication develops-convert immediately to surgical cricothyroidotomy. Stab incision via pores and skin and membrane, enlarge incision with blunt dissection. Difficult airway: Conclusions � the obstetrician and anesthesiologist ought to be alert to the presence of problematic airway. Proper positioning for oxygenation and intubation is crucial in parturients with tough airway. Repeated attempts at intubation are contraindicated after ineffective exterior laryngeal manipulation and progressive hypoxia [65]. The airway needs to be secured with alternative methods (see the inverted traffic gentle algorithm), and oxygenation should be maintained. Keep the exterior auditory meatus and the sternal notch in the same horizontal plan. This is best than the "sniff position" for alignment of the oral, pharyngeal, and laryngeal axes. The incidence of aspiration of gastric contents is extensively quoted to range from 1 in 900 to 1 in 1547 (0. A prospective observational study from Australia and New Zealand confirmed that regurgitation of gastric contents throughout basic anesthesia for cesarean delivery occurred in eight circumstances out of 1095 (0. Pregnant girl ought to be thought-about as "full abdomen" whatever the fasting status. However, of observe is the truth that once labor begins, a delay in gastric emptying happens [7]. The authors concluded that the efffects of interventions similar to administration of H2 receptor blockers and/or sodium citrate are less constant than previously believed. However, the authors concluded that their use ought to still be strongly considered [35]. Cerebrovascular stroke In addition to physiological adjustments during being pregnant, pregnancy-related problems such as preeclampsia and/ or eclampsia can contribute to the elevated incidence of cerebrovascular and intracranial opposed events during pregnancy, labor, and postpartum. Feske and Singhal reported that the incidence of all forms of strokes is 4 to seven cases in a hundred,000 pregnancies [68]. Lanska and Kryscio reported that cesarean supply was associated with a 3- to 12-fold elevated danger of peripartum and postpartum stroke [69]. Meticulous attention to the hemodynamic stability throughout common anesthesia, particularly in preeclamptic or eclamptic patients during the induction of anesthesia and intubation is essential to keep away from any intracranial opposed events. Intracranial hemorrhagic stroke Intracranial hemorrhage is the commonest cause of maternal demise from stroke in patients with preeclampsia or eclampsia [70]. Aspiration pneumonitis (Mendelson syndrome) Aspiration pneumonitis (Mendelson syndrome) and its mechanism beneath the settings of anesthesia for obstetric patients was first reported by an obstetrician-Dr Mendelson. We administer metoclopramide routinely, and H2 blocker in chosen instances, such as diabetes or morbid obesity, on prime of the antacid sodium citrate. Aspiration pneumonitis used to be one of the major causes of perioperative maternal demise. A variety of preventative measures have been launched over time to forestall this lethal situation. Rapid sequence induction approach with cricoid strain and use of sodium citrate and H2 blockers have decreased the incidence of aspiration of gastric contents [66]. References 319 problems together with coagulopathies; preeclampsia and eclampsia had been identified as the chance elements for intracranial hemorrhage [73]. Cardioembolism, preeclampsia or eclampsia (11%�47% of stroke cases), and cerebral venous sinus thrombosis account for many pregnancy-related ischemic strokes [68].
Cialis with dapoxetine 20/60mg cheap amexThe application of three-dimensional color energy Doppler ultrasound within the description of irregular uteroplacental angioarchitecture in placenta previa percreta erectile dysfunction forum cialis with dapoxetine 20/60 mg discount without prescription. In spite of routine uterotonics administration erectile dysfunction underwear cialis with dapoxetine 40/60mg discount on line, major obstetric hemorrhage is frequent, even in women who appear at low danger [2]. And any surgeon can get right into a state of affairs of discovering a pool of blood underneath the patient only after finishing the operation and removing surgical drapes. When the uterine incision is stitched, the uterine cavity instantly turns into dead area underneath the uterine seam. And this useless area might harbor each hid bleeding and blood clot accumulation. Intrauterine clots in addition to retained parts of placenta are well-known causes of hemorrhage. So the hid blood loss typically ends in dramatic delay in recognition of its severity and ill-timed remedy [4,5]. As main complications start in the uterine cavity after the stitching of the hysterotomic incision, a consequential reaction is to do one thing before the closure of the wound to avoid these problems. One easily comes to the idea of uterine cavity temporal occlusion, till clotting all probably bleeding vessels. After this maneuver the uterus should be left unaffected, without any bleeding and blood clots and with correct lochia discharge. Our idea of this uterine occlusion is to occupy the cavity immediately after emptying the uterus with a straightforward expandable thin-walled silicon balloon. But the safe placement of an increasing inflated balloon contained in the newly incised and stitched uterus is possible solely after we obey some clear, strict calls for. The balloon should 10 � Occupy entirely the whole cavity, overlaying all doubtlessly bleeding vessels. One of the vessels is a thin-walled simply expandable intrauterine balloon, and the second is a tank positioned at the required top above the balloon level. Both vessels are related with a quite broad tube that stays continuously open during the entire process. Receive visual details about uterine activity by the altering degree of solution in the tank. The Probe-Plug is an orange plastic stick: its size is 25 cm and its diameter is 5. It is flexible and gentle enough to avoid perforation or trauma of the uterus in the course of the insertion, and rigid sufficient to enable the internal cervical ostium to be discovered easily with out visual control. In some cases we might use the Probe-Plug as a plug for saving the solution within the balloon once we connect the vaginal balloon catheter. For this we take away the ProbePlug and join the catheter to the tank pre-filled with the warm resolution positioned half a meter above the affected person. To noticeably simplify this step, we created an auxiliary device specially designed for retrograde insertion of the balloon catheter. Its task is only to hold the answer within the uterine cavity and to forestall escape of the solution into the vagina and fallopian tubes. While the connecting tube stays open through the procedure, the balloon is able to react spontaneously on uterine contraction by changing its quantity. Adjusting the peak of the tank permits number of any required pressure on the uterine wall for any individual case. The first circumstances of utility revealed that achievement of intrauterine hemostasis requires surprisingly low stress (10�15 mm Hg). Our early experience revealed that even only a contact of uterine wall with the balloon is sufficient to obtain a preventive effect. In uncommon cases of blood leakage over the balloon, we are ready to arrest bleeding by raising the tank to increase the pressure. The method of making adequate counterpressure for holding the balloon in the cavity and conducting correct blood loss monitoring in the case of ongoing bleeding appears to not be practical. Even a temporal hemostasis is vitally essential to give time for a clinician, but typically we are in a position to obtain the finished one. Its purposes are to maintain the uterine balloon within the cavity and at the similar time make it attainable to detect uterine bleeding. The uterine balloon ought to be deflated slightly to fit the cavity and keep away from protruding. Thus the vaginal module is safely fixed within the higher part of the vagina, adjoining the underside facet of the intrauterine balloon. Any possibility of intrauterine balloon prolapse into the vagina throughout its refilling even with an open cervix is absolutely excluded. The hole permits blood and even clots to run freely out in case of uterine bleeding. Thus a surgeon is able to evaluating the effectiveness of applying this method. In reality, wide preventive utilization of the strategy gives large financial effect, as increasingly typically we handle to stop "near-miss" circumstances, and every of them costs $50,000�$70,000 for medical budget. The summarized calculation of bills after methodology implementation within the Tyumen region of the Russian Federation has revealed a $1. In cases the place the vascular system of the uterus was intact, the approach almost at all times works. Retrospective analysis of rare instances requiring surgical intervention showed that the integrity of the vascular system of the uterus had been damaged (uterine laceration, retained lobule of placenta accreta, congenital ailments of the uterine vessels, etc. Processing the outcomes, we found a dramatic discount in postpartum endometritis cases [8]. At this important moment nobody on the earth is ready to acknowledge the case with oncoming issues [6]. Endometritis Bacterial colonization of the uterine cavity is detected in 94% of postpartum sufferers, but only a small fraction truly develop the infection. In our opinion the function of blood clots trapped in the cavity of the uterus is underestimated. During the operation the blood often collects within the cavity and its discharge is impeded. Contractive operate of the incised uterus is insufficient, drainage of the cavity is poor, and the cervix incessantly is closed. The pathological contents saved within the uterus are inaccessible after closure of the incision. This inviable tissue trapped in the uterus very quickly becomes a nutrient medium for microbial growth. It is a properly known medical incontrovertible truth that after the evacuation of these contents the restoration is rapidly achieved. In our opinion, this might be possible because we prevented the accumulation of pathological contents by the balloon occlusion. Discussion Once retained products and genital tract trauma have been excluded, an obstetrician has only 4 options to provide intrauterine hemostasis: Uterotonics Some knowledge show that 10%�21% of women fail to respond to treatment with standard uterotonics [10]. When giving uterotonic remedy, the clinician often counts on a sufficient amount of muscle tissue being ready to reply, but in a number of cases (lower phase placentation, cicatricial changes of myometrium, and so on. But when the uterotonics fail the bleeding may be arrested with the intrauterine balloon.
Discount cialis with dapoxetine 20/60 mg on-lineSurvey on the adequacy of depth of anaesthesia with bispectral index and isolated forearm method in elective Caesarean section under common anaesthesia with sevoflurane erectile dysfunction effects 40/60 mg cialis with dapoxetine purchase otc. Maternal inspired oxygen focus and neonatal status for caesarean section under common anaesthesia erectile dysfunction 23 cialis with dapoxetine 20/60 mg order. Bispectral index monitoring to prevent consciousness during anaesthesia: the B-Aware randomised controlled trial. Risk elements for peripartum and postpartum stroke and intracranial venous thrombosis. Pregnancy-associated intracranial hemorrhage: Results of a survey of neurosurgical institutes across Japan. The majority of maternal deaths happen during administration of general anesthesia and end result from airway management-related complications. One of them is chosen primarily based on its traits, maternal preference, maternal common well being condition, and the indications. In contrast, the recognition of de novo epidural anesthesia for elective cesarean delivery is lowering (somewhat less reliable and currying higher danger of native anesthetic toxicity). In the past, epidural anesthesia was believed to be superior to spinal anesthesia for a parturient with preeclampsia as a outcome of its slow onset guaranteed more hemodynamic stability. However, several studies have proven that the hemodynamic effects of spinal anesthesia are just like those of epidural method [4,5] (Table 19. In the United States more than 30% of parturients presenting for obstetric anesthesia are chubby and/or overweight. In the overweight sufferers, the spinal needle will not be advanced straight and simply into the subarachnoid house, as a outcome of the gap from skin to the subarachnoid area is much longer than in nonobese parturients. Once epidural house is recognized with a lack of resistance approach, the spinal needle could also be easily advanced via the epidural needle. Prior to the initiation of epidural anesthesia, the degree of the residual spinal anesthetic results should be thought-about. Hence, spinal needle insertion should be performed at L2/3 or more caudal interspaces to be able to keep away from direct trauma to the spinal wire. The primary constituents within the subarachnoid house at this degree are cerebral spinal fluid, cauda equina, and blood vessels. The arachnoid and the dura matter constitute the outer layer of the subarachnoid space. Surrounding the dura matter is the epidural area, the dorsal part of which is used for epidural anesthesia. The ligamentum flavum, the necessary thing structure to identify the epidural space, is positioned immediately dorsal to it. An epidural catheter for cesarean supply is normally positioned through L3/4 or L4/5 in order that T4�S5, the necessary block range for the surgical procedure, is successfully blocked. The use of lidocaine must be withheld due to concerns about neurotoxicity. Whichever agent is chosen, a hyperbaric anesthetic is mostly chosen for cesarean delivery. Hence, block to T4 dermatome is extra quickly achieved with hyperbaric solutions of native anesthetics. L4 Fentanyl or sufentanil (most in style opioids in obstetrics) are generally added to the native anesthetic agent. These opioids are identified to prolong duration of anesthetic results and also decrease intraoperative nausea and vomiting. Therefore, morphine is usually administered along with either of the short-acting opioids. Side results of intrathecal morphine include postoperative nausea/vomiting, pruritus, and delayed respiratory depression. Therefore, respiratory fee and pulse oximetry ought to be monitored for no less than 24 hours after administration of intrathecal (spinal) morphine. It should be noted that nerve roots inside the subarachnoid area are extremely susceptible to chemical harm. Caution must be exercised to keep away from contamination of subarachnoid injectate with preservatives. Epidural anesthesia Local anesthetic used for epidural anesthesia is just like that used for spinal anesthesia, but the epidural dose is much larger than the spinal dose. The drug selections for elective cesarean supply or extension of epidural labor analgesia for nonurgent cesarean deliveries embody zero. Levobupivacaine and ropivacaine are relatively new L- or S-isomer brokers, resulting in less potential for cardiotoxicity. The alkalization of local anesthetic by sodium bicarbonate not solely shortens the onset of blockade but in addition improves its high quality, and prolongs the duration of the blockade. Alkalization increases the nonionized type of native anesthetic molecules, which pass extra easily through the neuronal membrane than ionized molecules. When choosing an appropriate anesthetic agent you will need to remember that the duration of motion of chloroprocaine and lidocaine is shorter than the length of motion of bupivacaine, levobupivacaine, and ropivacaine. Subsequently, top-up boluses could also be essential throughout surgery when both chloroprocaine or lidocaine is chosen. Neuraxial opioids are sometimes mixed with local anesthetic so as to shorten the onset of anesthesia, and improve and delay the duration of surgical anesthesia. One meta-analysis confirmed that 100 mcg fentanyl mixed with 2% lidocaine, or seventy five mcg fentanyl mixed with levobupivacaine shortened (by 2 minutes) the onset of surgical anesthesia [13]. The examine in question additionally demonstrated that a mix of lidocaine and epinephrine, with or with out fentanyl, shortened the onset of surgical anesthesia. These neuraxial opioids have unwanted side effects, such as pruritus, nausea and vomiting, delayed gastric emptying, urinary retention, sedation, and respiratory despair. Morphine-induced respiratory depression is often minimal, but may be life threatening. Therefore, the patient who acquired epidural morphine must be repeatedly monitored (with pulse oximetry) for at least 24 hours after morphine administration. Selection of local anesthetics and opioids is equivalent to what has been outlined above for every approach when used alone. Pre-anesthetic evaluation As outlined in Practice Advisory published by the American Society of Anesthesiologists [15] an in depth maternal medical and anesthetic historical past, medications, allergy symptoms, laboratory knowledge, and baseline blood stress and heart fee should be obtained previous to anesthesia. Physical examination includes evaluation of airway (please see Chapter 18, "General Anesthesia for Cesarean Delivery: Indications and Complications"), heart, and lungs. For neuraxial anesthesia, shut consideration should be paid to maternal coagulation status and the needle insertion web site (evaluation of the back area) [16,17]. Coagulopathy is among the contraindications to neuraxial anesthesia, as it may end up in epidural hematoma. Anatomical disorder, an infection, and neoplasms on the website of needle insertion could additionally be contraindications to neuraxial technique [21]. When sensory nerves are blocked by neuraxial anesthesia, sympathetic nerves are also blocked, resulting in vasodilation. This causes hypotension, which requires aggressive and prompt treatment to keep away from maternal and fetal problems. Anesthesia-related hypotension is aggravated by pre-existing hypovolemia [1,7,8,14].
Cialis with dapoxetine 40/60 mg buy without prescriptionFirst erectile dysfunction after prostate surgery cialis with dapoxetine 40/60mg discount on line, one retrieves the remaining FiberTape limbs from every medial anchor and the anterior cinch stitch into the anterolateral portal erectile dysfunction drugs prostate cancer cialis with dapoxetine 20/60 mg order on line. The SwiveLock Anchor is loaded with the two remaining FiberTape limbs and the anterior cinch sew. These are tensioned for even rotator cuff reduction to the footprint, and the SwiveLock is totally seated. The variety of lateral row anchors used is often the same as the number of medial row anchors. C, Four sutures from the medial row, after knot tying, are incorporated into every of the two lateral row anchors. Four mattress knots tied alongside the medial row (from two medial row anchors) with sutures included into two lateral row anchors. The affected person stays in a postoperative sling with a small abduction pillow always for 6 weeks. At 6 weeks, the affected person is allowed to begin shoulder active-assisted and passive vary of movement with outpatient bodily therapy. At 12 weeks, energetic motion and mild strengthening are begun with outpatient bodily remedy. Patients are then seen at 6 weeks after surgery to initiate outpatient bodily remedy. The subsequent appointment is at 12 weeks to assess vary of movement and start rotator cuff strengthening. Patients then are seen at 6 months, at which point they need to be getting near returning to regular actions. Arthroscopic restore of full-thickness rotator cuff tears with and without acromioplasty: randomized prospective trial with 2-year follow-up. A potential randomized scientific trial comparing arthroscopic single- and double-row rotator cuff restore: magnetic resonance imaging and early scientific evaluation. Prospective randomized study of arthroscopic rotator cuff repair using an early versus delayed postoperative physical therapy protocol. Equivalent medical results of arthroscopic single-row and double-row suture anchor repair for rotator cuff tears: a randomized managed trial. The end result and restore integrity of fully arthroscopically repaired giant and massive rotator cuff tears. For outpatient rotator cuff surgical procedure, nerve block anesthesia provides superior same-day recovery over general anesthesia. A multicenter randomized managed trial evaluating single-row with double-row fixation in arthroscopic rotator cuff repair. Arthroscopic rotator cuff repair with and without acromioplasty within the remedy of full-thickness rotator cuff tears: a multicenter, randomized controlled trial. Clinical consequence in all-arthroscopic versus mini-open rotator cuff restore in small to medium-sized tears: a randomized managed trial in 100 patients with 1-year follow-up. However, it was not till 1977, when descriptions of the arthroscopic therapy of pediatric congenital hip dislocations appeared, that the method began to achieve reputation. The sluggish development of hip arthroscopy has been attributed to each difficulties navigating the anatomic constraints surrounding the hip and the delayed recognition of anatomic abnormalities of the hip by surgeons. Refinements in the understanding of hip pathology, diagnostic imaging, and arthroscopic instrumentation have facilitated the fast expansion of hip arthroscopy to prognosis and deal with disorders of the hip. With the developments seen in the past decade, there was a surge in the usage of arthroscopy in the treatment of hip problems. The differential prognosis of ache about the hip is extensive and traditionally has introduced a diagnostic dilemma. Consideration have to be given to direct, oblique, and sports hernias; retroperitoneal or intraabdominal pathology; gynecologic pain; central or peripheral nervous system contributions; and lumbar, sacral, and pelvic pathology. When the signs localize to the hip, it turns into imperative to delineate between intraarticular and extraarticular hip etiology. Postural abnormalities include pelvic obliquity and tilt, leg size discrepancy, scoliosis, and lordosis. Examination of the hip joint consists of careful palpation of all associated buildings. Tenderness in the adductor or psoas tendons, hip flexor or rectus abdominus musculature, higher trochanteric bursa, or hamstring origin could additionally be an indicator of primary pathology or secondary signs from an intraarticular abnormality. Active and passive vary of motion in each hips must be evaluated for any asymmetry. Provocative tests can assist with the identification of particular hip abnormalities. An anterior impingement check elicits ache with passive hip flexion, adduction, and inside rotation. This may be indicative of intraarticular pathology that involves the acetabular rim, labrum, or femoral head-neck junction. A posterior impingement take a look at is carried out with the hip ready of extension and exterior rotation. Pain is brought on when the femoral head-neck junction impinges on the posterior acetabulum and labrum. This take a look at might help diagnose impingement when compared with the nonsymptomatic hip. A dial test could reveal elevated movement in the hip within the presence of hip instability. The presence of either coxa profunda or protrusio acetabuli is a sign of acetabular overcoverage. The presence of acetabular retroversion is determined by figuring out a crossover sign or outstanding extension of the ischial backbone into the pelvis. A posterior wall sign, current when the posterior acetabular wall lies medial to the middle of the femoral head, can also be indicative of acetabular retroversion. The presence of dysplasia and threat of instability could be higher understood by figuring out acetabular inclination. This is done with measurement of the Tonnis, the sharp, and the lateral center edge angles. The cross-table lateral view is assessed for the presence of cam-type impingement, femoral head sphericity, and femoral head neck offset. The alpha angle is typically considered positive for cam impingement with values over 50 levels. This angle additionally has been shown to give predictive info for the probability of concomitant chondrolabral harm and identification of those with a hip in danger for future symptoms. The monitor is positioned in the direct visible subject with the assessory screens positioned for the assistant. Pay attention to the location of fluroscopy from the contralateral facet, surgical lights, and multiple tables, if required. The operative hip is positioned to impartial, making a lateralizing drive to the femur over the publish. Access to the operative website is covered with occlusive dressing to forestall fluid egress and ingress about the surgical area. The nonsterile assistant ought to have access to the decrease extremity to manipulate the extremity while permitting the surgeon to assess the situation of the extremity.
|