15 mg mobic order with amexTreatment is typically surgical and contains stabilization with plates and/or screws arthritis in fingers pregnancy mobic 15 mg buy mastercard, or by substitute of the femoral head (hemiarthroplasty) or whole hip substitute arthritis in fingers and knees generic mobic 7.5 mg with amex. Treatment of the illness with bisphosphonates can scale back ache, but coexistent osteoarthritis of the hip can even happen. Avascular necrosis Segmental avascular necrosis of the weight-bearing portion of the femoral head can occur. Management of hip pain the most important step in administration of the painful hip is to set up the underlying aetiology and to treat it as particularly as possible. Thus infection of the hip should be diagnosed expeditiously and treated with surgical drainage and prolonged parenteral antibiotics. Here we current a couple of general rules that apply to the management of hip pain due to any variety of aetiologies. First, a cane may be extraordinarily useful in unloading the painful hip and relieving pain. Second, as with most other joints, the hip can become stiff with disuse and develop flexion contractures. Finally, you will want to recognize that one musculoskeletal problem can result in another. Patients with spinal stenosis incessantly develop trochanteric bursitis, for example. The picture on the prime left shows a small acetabular labral tear Ischial bursitis-The ischial bursa separates the gluteus maximus from the ischial tuberosity. Meralgia paraesthetica-This situation refers to native compression of the lateral cutaneous femoral nerve (L2-3 distribution) at the inguinal ligament. The syndrome is felt to come up from direct compression of the nerve; hence, weight problems, being pregnant, tight-fitting belts and waistbands and hip extension (as can occur with high heels) are danger components, as is diabetes mellitus. The syndrome usually improves with conservative measures such as weight reduction, and modifications in clothing and sneakers. Torn acetabular labrum-This produces ache in the groin on rotatory movements of the hip, and the hip might feel unstable or give Further studying McRae R. Most knee accidents in sport happen on account of indirect trauma, corresponding to a twisting moment to the knee. The buildings mostly injured by this mechanism are the menisci, the collateral ligaments and the cruciate ligaments. Direct trauma to the knee (such as during contact sport, an industrial accident or a motor-vehicle collision) most commonly causes bone contusions, fracture or dislocation which will have an result on the patello-femoral or tibio-femoral joint. Dislocation of the tibio-femoral joint signifies high-energy trauma, and is often related to neurovascular harm. Knee movement occurs in a fancy manner involving three planes, though the vast majority of its motion occurs in the sagittal airplane (from full extension through to a hundred and forty � of flexion). Pain within the knee joint is among the most typical musculoskeletal complaints that presents to primary care physicians, and will arise from a broad vary of pathologies. In the younger affected person, ache most commonly arises from sporting or overuse accidents, which can have an effect on the intra-articular or extra-articular structures of the knee. Knee pain arising from osteoarthritis is a significant cause of incapacity within the older patient, the prevalence and health-care prices of which continue to rise as the population ages. Meniscus injury Meniscus harm in young people can current as an acute harm or as a continual situation with an insidious onset. The majority of meniscus tears in younger people happen after mild- to moderateenergy twisting injuries and are typically isolated injuries or related to a collateral ligament strain. Higher-energy twisting injuries are commonly associated with an anterior cruciate ligament damage, an acute haemarthrosis and inability to bear weight. Patients with meniscus tears have focal tenderness over the joint line and may experience mechanical catching and locking symptoms in the knee in addition to joint effusion and pain. Acute tears that happen in the well-vascularized peripheral portion of the meniscus are amenable to arthroscopic repair, which preserves meniscus perform. Where an anterior cruciate ligament harm is also current this is reconstructed concurrently. Arthroscopic resection is confined to the torn and degenerate parts of meniscus, as early-onset osteoarthritis of the knee generally follows full meniscal resection. Occult episodes of trauma to the knee might end in separation of cartilage from the subchondral bone, termed osteochondritis dissecans. A detailed history of the mechanism of damage and bodily examination provide useful data to differentiate between the assorted traumatic causes of knee ache. Knee ache from injury has a sudden onset at the time of the damage episode and is commonly accompanied by native soft-tissue swelling and an effusion. Certain fractures and dislocations could exhibit gross deformity; nonetheless, the vast majority of knee and patellar dislocations spontaneously reduce earlier than presentation. A haemarthrosis develops quickly (over a interval of minutes to a few hours) and signifies significant intraarticular injury, corresponding to an anterior cruciate ligament tear, intraarticular fracture or osteochondral injury, or patellar dislocation. Effusions, which develop over several hours, tend to be related to meniscal accidents (Table 6. Radiographs must be obtained when evaluating any knee injury to exclude a fracture, dislocation or other vital abnormality. In the absence of neurovascular compromise or gross deformity, initial therapy of traumatic knee ache ought to consist of restricted weight bearing, ice and elevation. The anterior part of the medial meniscus may be seen as a black triangle on the left side of the joint line; the black triangle of the posterior a half of the meniscus has a white line running via it, representing an indirect tear Knee ache in youthful individuals and athletes may be attributable to overuse syndromes, meniscus injury or articular cartilage abnormality. Common overuse syndromes embrace patellar tendonopathy, anterior knee pain syndrome, pes anserine bursitis and iliotibial band friction syndrome (Table 6. Articular cartilage accidents can lead to focal pain, joint effusion and mechanical catching symptoms. Treatment comprises graduated physiotherapy for undisplaced injuries and arthroscopic restore or Patellar tendonopathy Patellar tendonopathy is brought on by repetitive exercise, notably "explosive" athletics similar to jumping. Treatment consists of ice, painrelieving medicine, activity modification and strengthening exercises specializing in eccentric loading of the tendon. Anterior knee ache syndrome Anterior knee pain syndrome happens in patients who engage in repetitive athletic activity, in these with abnormalities in extensor mechanism alignment and in those who are chubby. Patients with anterior knee pain syndrome complain of pain in the front of the knee, which is accentuated by ascending and descending stairs, squatting, kneeling and by sitting for long durations of time. The ache could also be positioned immediately behind the patella or in the medial or lateral retinaculum. Treatment ought to include exercise modification, weight control if necessary, physiotherapy to strengthen the quadriceps muscles (particularly vastus medialis) and core musculature, and applicable pain-relieving medicine. Pes anserine bursitis Pes anserine bursitis is an irritation of the bursa overlying the insertion web site of the semitendinosus, gracilis and sartorius tendons in the anteromedial facet of the proximal tibia. Treatment can embrace exercise modification, strengthening exercises and antiinflammatory medicine. Iliotibial band friction syndrome Iliotibial band friction syndrome is an irritation of the iliotibial band, the distal portion of the tensor fascia lata muscle that inserts into the anterolateral facet of the proximal tibia. Patients are usually runners or cyclists who complain of activity-related lateral knee pain. This situation responds properly to activity modification, stretching and strengthening exercises, ice and anti-inflammatory drugs.
Mobic 15 mg purchase otcTwo of those areas are tissue mass referred to as nodes; the third is a gaggle of fibers called the atrioventricular bundle arthritis research back exercises mobic 7.5 mg buy generic on line. The sinoatrial node psoriatic arthritis in the knee generic mobic 15 mg free shipping, which is located I the upper wall of the best atrium an initiates the guts beat, known as the pacemaker. The second node, located within the ineratrial septum at the bottom of the proper atrium, is known as the atrioventricular node. The atrioventricular bundle, also referred to as the bundle of His, is positioned on the top of the interventricular septum; it has branches that extend to all components of the ventricle partitions. Fibers travel first down either side of the interventricular septum in groups called the best and left bundle branches. The relatively slower conduction through this node allows time for the atria to contract and full the filling of the ventricles. The excitation wave travels rapidly via the bundle of His after which all through the ventricular partitions via the bundle branches and Purkinje fibers. As a security measure, a area of the conduction system apart from the sinoatrial node fails, nevertheless it does so at a slower fee. Recall from chapter 7 that stimulation from the sympathetic nervous system increases the guts price and the stimulation from the parasympathetic nervous system decreases the heartrate. The heart fee is also affected by such elements as hormones, ions, and medicines within the blood. Sinus arrhythmia is a daily variation in heart rate because of changes in the price and depth of breathing. Premature beats, also known as extrasystoles are beats that are available earlier than the the expected normal beats. They could happen in regular individuals initiated by caffeine, nicotine, or psycologic stresses. It is probably brought on by a mix of issues, together with closure of the atrioventricular valves. It happens at the beginning of ventricular rest and is due in giant part to sudden closure of the semilunar valves. Some abnormal sounds called murmurs are normally because of faulty action of the valves. For instance, if the valves fail to close tightly and blood leaks back, a murmur is heard. Another situation giving rise to an irregular sound is the narrowing (stenosis) of a valve opening. The many situations that may cause abnormal coronary heart sounds include congenital defects, disease, and physiological variations. An abnormal sound attributable to any structural change within the heart or the vessels connected with the heart is identified as an organic murmur. Blood Vessels Functional classification the blood vessels, along with the four chambers of the guts, from a closed system for the flow of blood; only if there 269 Human Anatomy and Physiology is an harm to some part of the wall of this technique does any blood escape. Arteries carry blood from the ventricles (pumping chambers) of the guts out to the capillaries in organs and tissue. Veins drain capillaries in the tissues and organs and return the blood to the center. Capillaries permit for exchanges between the blood and physique cells, or between the blood and air in the lung tissues. Note smooth muscle is discovered in the center layer or tunica media of arteries and veins. In arteries, the tunica medial performs a critical position in sustaining blood pressure and controlling blood distribution within the body. A thin layer of elastic and white fibrous tissue covers an inner layer of endothelial cells called the tunica interna in arteries and veins. The tunica interna is definitely a single layer of squamous epithelial cells referred to as endothelium that lines the internal surface of the whole circulatory system. The most essential structural characteristic of capillaries is their excessive thinness-only one layer of flat, endothelial cells composes the capillary membrane. Instead of three layers or coats, the capillary wall consists of solely one-the tunica interna. Substances similar to glucose, oxygen, and wastes can shortly pass through it on their way to or from the cells. Smooth muscle cells which would possibly be known as precapillary sphincters guard the entrance to the capillary and decide into which capillary blood will flow. The thoracic aorta lies simply in front of the vertebral column behind the guts and within the house behind the pleura. The belly aorta is the longest part of the aorta, spanning the belly cavity. Sections of small blood vessels displaying the thick arterial walls and the thin walls of veins and capillaries. These from a crown across the base of the guts and provides off branches to all elements of the myocardium. Branches of the Aortic Arch the arch of aorta, located immediately beyond the ascending aorta, provides off three giant branches. After extending upward somewhat less than 5 cm (2 inches), it divides into the best subclavian artery, which provides the best facet of the pinnacle and the neck. The left common carotid artery extends upward from the best part of the aortic arch. The left subclavian artery extends underneath the left collar bone (clavicle) and supplies the left upper extremity. Branches of the Thoracic Aorta the third a part of the aorta supplies branches to the chest wall, to the esophagus, and to the bronchi and their treelike subdivisions in the lungs. There are often 9 to ten pairs of intercostal 274 Human Anatomy and Physiology arteries that extend between the ribs, sending branches to the muscular tissues and other structures of the chest wall. Branches of the Abdominal Aorta As within the case of the thoracic aorta, there are unpaired branches extending forward and paired arteries extending toward the aspect. The superior mesenteric artery, the biggest of these branches, carries blood to a lot of the small intestine as properly as to the first half of the big gut. The much smaller inferior mesenteric artery, positioned under the superior mesenteric and close to the tip of the belly aorta, supplies the second one half of the large intestine. The lateral (paired) branches of the belly aorta include the following proper and left divisions: 1. The ovarian arteries within the female and testicular arteries in the male (formerly referred to as the spermatic arteries), provide the intercourse glands. The pulmonary veins carry oxygenated blood from the lungs to the left atrium of the guts. Both of these vessels, about 5 cm lengthy, lengthen into 277 Human Anatomy and Physiology the pelvis, the place every one subdivides into an internal and an external iliac artery. The internal iliac vessels then send branches to the pelvic organs, including the urinary bladder, the rectum, and a few of the reproductive organs. These vessels give off branches within the thigh and then turn into the popliteal arteries, which subdivide below the knee.
7.5 mg mobic cheap free shippingGlobal issues the problems discussed on this chapter have global utility arthritis pain left arm purchase mobic 7.5 mg with amex, as the burden of sickness from musculoskeletal conditions is excessive in each the developed world and developing nations alike arthritis in fingers and diet cheap mobic 15 mg with amex, significantly with an ever-increasing aged inhabitants worldwide. Awareness of the importance of musculoskeletal circumstances, when it comes to morbidity but in addition mortality, must be raised amongst all health-care employees, governments and members of the basic public. With growing journey and migration, information of the worldwide spectrum of musculoskeletal conditions is necessary. There additionally must be an increasing emphasis on prevention through encouraging wholesome existence and joint protection and by tackling modifiable threat factors corresponding to falls prevention. Conclusion Over the last 10 years there was a shift in serious about how greatest to take care of patients with rheumatological problems (Box 1. For those with inflammatory arthritis the emphasis is on immediate referral to secondary care in order that treatment with probably disease-modifying agents could be instituted early, before irreversible joint injury has occurred. Remember to ask about precipitating factors, especially work/ occupation and hobbies. Hand or wrist pain and resultant impaired function are sometimes the reason for nice anxiety for sufferers. Hands, as prehensile organs, give us a nice deal of information about the world by which we live. They are capable of performing incredibly fine and delicate actions and are essential for work, sport, hobbies and social interaction. The eight carpal bones, in two rows of four, kind a bony gutter and are the base of the carpal tunnel. The flexor retinaculum, a robust fascial band, forms the palmar facet of the tunnel. Running by way of the carpal tunnel are the deep and superficial flexor tendons, the tendons of flexor pollicis longus, flexor carpi radialis and the median nerve. The extensor tendons are held in place on the extensor surface of the wrist by the extensor retinaculum. All of the flexor tendons are encased in a common synovial tendon, which extends from a place simply proximal to the wrist to the center of the palm. Flexor pollicis longus and flexor carpi ulnaris have their own individual sheaths, as do each of the six extensor compartments. The hand bones are the metacarpals, proximal phalanges, middle phalanges, distal phalanges and sesamoid bones. A sesamoid bone lies at the base of the thumb within the tendons of flexor pollicis brevis. The first metacarpal bone of the thumb is the shortest and most cell of the metacarpals and lies in a different airplane to the others. Individual tendon sheaths for the deep and superficial flexor tendons start on the level of the distal transverse crease of the palm and finish on the bases of the distal phalanxes. The sheath for flexor pollicis longus continues from the carpal tunnel to the distal phalanx. During flexion, five fibrous bands, or pulleys, hold the flexor sheaths in place. Passive extension varies from 60 � to greater than one hundred � in individuals with hypermobility. The lumbrical and interossei muscles produce complicated movements that involve extension of the interphalangeal joints and flexion on the metacarpophalangeal joints and are essential to nice hand functions, such as writing. Local anaesthetic helps introduce the needle alongside the tendon within the palm simply proximal to the metacarpophalangeal joint. Repetitive use of the hand will increase the chance of creating carpal tunnel syndrome however its standing as a piece harm is controversial (Yagev et al. A ganglion, or very hardly ever amyloidosis or myxoedema, causes carpal tunnel syndrome. Pain, tingling and numbness in a median nerve distribution (thumb, index finger, middle and radial facet of ring finger) are typically present on waking or can wake the affected person. The symptoms could appear when the patient holds a newspaper or the steering wheel of a car. Permanent numbness and losing of the thenar eminence (flexor pollicis and opponens pollicis) cause clumsiness. Weakness of abduction of the thumb distal phalanx with the thumb adducted towards the fifth digit is typical. Management and injection technique-A splint worn on the wrist at night time relieves or reduces the symptoms of carpal tunnel syndrome. The needle is inserted at the distal wrist pores and skin crease, just to the ulnar aspect of the palmaris longus tendon, or about 0. If a small check injection of corticosteroid causes finger pain, the needle is in the nerve and must be repositioned. Recurrent daytime symptoms, unrelieved by splints, warrant nerve-conduction research. Slowing of median nerve conduction on the wrist suggests demyelination as a end result of native compression. The motion potential is lowered or absent due to nerve-fibre loss if the lesion is severe or prolonged. Decompression surgical procedure should be thought-about for: recurrent symptoms not eased by splints or injection; significant nerve injury; muscle wasting; and/or everlasting numbness (Trumble et al. Recovery of sensation or energy, or each, could also be limited or non-existent if the lesion is extreme and longstanding. Overuse and local damage (after opening a decent jar) are the commonest causes of thumb flexor tenosynovitis and trigger thumb. Corticosteroid injection next to the sesamoid bone at the site of maximal tenderness helps. Finger flexor tendonosis and trigger finger Gripping and hard manual work trigger palpable thickening and nodularity of the finger flexor tendon; tendon sheath synovitis can also be present. The affected fingers are stiff in the morning, when the affected person also has ache within the palm and along the dorsum of the finger(s). This is frequent in rheumatoid arthritis and in dactylitis caused by seronegative arthritis. Nodular flexor tenosynovitis is extra common and less responsive to therapy in sufferers with diabetes than in different sufferers (Stahl et al. Trigger finger is caused by a nodule catching at the pulley that overlies the metacarpophalangeal joint in the palm. The affected person wakens with the finger flexed and has to force it straight with a painful or painless click. It causes ache at or simply proximal or distal to the styloid, in distinction with first carpometacarpal osteoarthritis, which causes pain at the base of the thumb. Management and injection technique-Rest is essential, with avoidance of thumb extension and pinching, but immobilization splints are inconvenient. The extensor retinaculum causes a typical "hourglass" form proximal and distal to the wrist. This contrasts with wrist synovitis, which causes diffuse swelling distal to the radius and ulna.
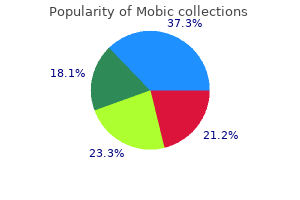
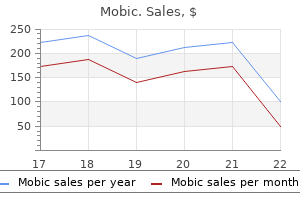
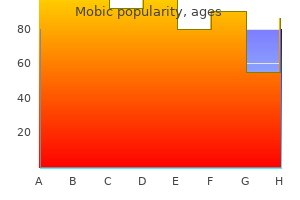
| Comparative prices of Mobic | | # | Retailer | Average price | | 1 | Kroger | 785 | | 2 | Price Chopper Supermkts | 710 | | 3 | Toys "R" Us | 118 | | 4 | Office Depot | 458 | | 5 | Ruddick Corp. | 364 |
Mobic 7.5 mg buy cheap lineIt is about 1 � inch lengthy and is discovered within the anal triangle that was described with the perineum arthritis muscle pain relief mobic 15 mg buy generic on-line. Note in each female and male arthritis pain relief liquid buy mobic 15 mg low cost, the anal canal is certain laterally by the fat-filled ischiorectal fossae and posteriorly by the anococcygeal body. Anteriorly, in the male, observe the perineal physique, the urogenital diaphragm, the membranous part of the urethra and the bulb of the penis. Anteriorly, within the female, observe the presence of the perineal physique, the urogenital diaphragm and the decrease a part of the vagina. The anal canal is composed of a longitudinal layer (continuation of the longitudinal layer of the rectum with fibers from the levator ani muscles) and a round layer. Based on embryological origin, the lining of the mucous membrane of the anal canal could be divided in two components, the higher half, derived from the hindgut endoderm and the lower part, derived from the ectoderm of the proctodeum. Note that the pectinate (dentate) line separates the upper from the lower anal canal. The higher part is lined by columnar epithelium, has anal columns, anal valves and anal crypts. The lower half has stratified epithelium (progressively merging with the perianal dermis on the anus), no anal columns and related structures. The anal canal has two sphincters, an involuntary internal sphincter and a voluntary exterior sphincter. Note that the puborectalis (part of the levator ani) blends with the deep a half of the external sphincter. Recall that the puborectalis muscle varieties a sling passing on the junction of the rectum and the anal canal. The exterior sphincter could be divided in three components: a subcutaneous half found at the lowest aspect of the anal canal, a superficial half attached posteriorly to the coccyx and anteriorly to the perianal body, and the deep part, situated on the higher finish of the anal canal. Note that the inner and the 3 parts of the external sphincter kind collectively an anorectal ring that could be discovered on rectal examination. The blood supply to the upper a half of the anal canal is by the superior rectal artery (branch of the inferior mesenteric artery). The blood supply to the lower portion of the anal canal is by the inferior rectal artery (branch of the interior pudendal artery). The venous return of the upper portion of the anal canal is by the superior rectal vein draining into the inferior mesenteric vein after which into the portal vein. The venous drainage of the lower a half of the anal canal is by the inferior rectal vein draining into the internal iliac vein and then the inferior vena cava. Recall that any important enhance in blood strain within the portal-systemic anastomosis because of liver disease can result in inner or external hemorrhoids. In terms of sensory innervation, note that the mucous membrane of the higher a half of the anal canal is innervated by sensory fibers ascending via the proper and left hypogastric plexuses. The lower portion of the anal canal is innervated by sensory fibers ascending through the inferior rectal nerves (branches of the pudendal nerve). In terms of motor innervation, the muscle fibers of the internal sphincter obtain sympathetic innervation from the hypogastric plexuses whereas the voluntary exterior sphincter is innervated by the inferior rectal nerve. The lymphatic drainage of the upper part of the anal canal is within the pararectal nodes after which in the inferior mesenteric nodes. The urinary bladder is discovered immediately posterior to the pubic symphysis in both male and female. The bladder has a powerful muscular wall and is ready to receive about 500 ml of urine. This muscular wall consists of three layers of clean muscle collectively often identified as the detrusor muscle. Note that though positioned in the pelvis, the bladder could be palpated through the anterior stomach wall, immediately above the pubic symphysis, when completely full. Classically, the bladder is described as having a pyramidal form, has an apex (connected to the umbilicus by the median umbilical ligament, a remnant of the urachus), a base (triangular posterior surface), and a neck (inferiorly). Note that the neck opens in the urethra (prostatic urethra in male) and that on the neck, the circular muscular fibers thickened to kind the sphincter vesicae. This sphincter, under autonomic management, regulates the release of urine from the bladder. Observe additionally that the neck is anchored to the walls of the pelvis by the pubovesical ligaments in female and puboprostatic ligament in male. The inside of the bladder muscular wall is covered by a mucous membrane forming folds in the empty bladder. The easy portion of the mucous membrane discovered beneath a line passing between the 2 ureteric orifices on the posterior wall is called the trigone. The superior surface and the higher a half of the posterior surface of the bladder is covered by peritoneum. Note that in feminine, the neck of the bladder (inferiorly) rests on the upper floor of the urogenital diaphragm whereas in male the neck of the bladder lies on the upper floor of the prostate. Laterally, in both the male and the feminine, the inferolateral surfaces are related anteriorly to the retropubic fat pads and posteriorly to the obturator internus above and the levator ani under. Note that in males, the 2 vas deferens and the two seminal vesicles could be found on the inferior facet of the posterior floor of the bladder, superior to the prostate (see later in this lecture). The superior and inferior vesical arteries (branches of the inner iliac arteries) present blood supply to the bladder in each women and men. In each males and females, the venous drainage is by the vesical venous plexus draining into the interior iliac vein through the superior and inferior vesical veins. Note that in males, the vesical venous plexus communicates with the prostatic venous plexus. In phrases of innervation, the bladder is beneath the management of the inferior hypogastric plexuses. The sympathetic fibers originate from the first and second lumbar ganglion, synapse in the inferior hypogastric plexuses and finish in the bladder. They inhibit contraction of the detrusor and stimulate the closure of the sphincter vesicae. The parasympathetic fibers move through the pelvic splanchnic nerves (S2-4), and also synapse in the inferior hypogastric plexuses before innervating the bladder. They stimulate contraction of the muscular wall and inhibit the motion of the sphincter vesicae. Most of the afferent (sensory) fibers are believed to attain the central nervous system through the pelvic splanchnic nerves, with only a few passing via the sympathetic fibers (1st and 2nd lumbar splanchnic). This muscle, innervated by the perineal branch of the pudendal nerve, compresses the urethra to cease the flow of urine out of the bladder. In male, as already mentioned, the urethra is divided in 3 parts, the prostatic, membranous and penile urethra. Beginning on the neck of the bladder, it passes via the prostate after which becomes the membranous urethra.
Mobic 15 mg buy on lineIn addition arthritis diet oatmeal buy mobic 7.5 mg free shipping, specialized cells in connective tissue defend the physique from microorganisms that enter the physique arthritis toes mobic 15 mg discount on line. Transport of fluid, vitamins, waste, and chemical messengers is ensured by specialised fluid connective tissues, such as blood and lymph. Finally, adipose cells retailer surplus vitality within the form of fats and contribute to the thermal insulation of the body. Unlike epithelial tissue, which consists of cells closely full of little or no extracellular area in between, connective tissue cells are dispersed in a matrix. The matrix usually consists of a great amount of extracellular material produced by the connective tissue cells which are embedded within it and performs a serious position in the perform of the tissue. The ground substance can vary from a watery fluid in blood, to a dense gel in cartilage, and even a mineralized matrix in bones. The quantity and construction of each part correlates with the perform of the tissue, from the inflexible ground substance in bones supporting the physique to the inclusion of specialized cells; for instance, a phagocytic cell that engulfs pathogens and likewise rids tissue of cellular particles. The three broad classes of connective tissue are classified based on the traits of their ground substance and the kinds of fibers discovered inside the matrix (Table three. Both tissues have a big selection of cell sorts (mesenchymal cells, fibroblasts, fibrocytes, adipocytes, macrophages, lymphocytes, and mast cells) and protein fibers (collagen, elastic, and reticular) suspended in a viscous floor substance. Dense connective tissue is reinforced by bundles of fibers that provide tensile power, elasticity, and safety. In free connective tissue, the fibers are loosely organized, leaving giant spaces between constructions. Loose Connective Tissue Loose connective tissue is discovered between many organs where it acts both to absorb shock and bind tissues together. It allows water, salts, and varied vitamins to diffuse through to adjoining or embedded cells and tissues. It fills the areas between muscle fibers, surrounds blood and lymph vessels, and helps organs in the stomach cavity. Areolar tissue underlies most epithelia and represents the connective tissue component of epithelial membranes. A giant number of capillaries permit speedy storage and mobilization of lipid molecules. White adipose tissue is most ample and seems yellow as a outcome of carotene and related pigments from plant meals. White fat contributes principally to lipid storage and may function insulation from chilly temperatures and mechanical injuries. White adipose tissue could be found protecting the kidneys and cushioning the back of the eye. Reticular cells produce the reticular fibers that type the community onto which different cells attach. Ligaments and muscle tendons are manufactured from dense common connective tissue, though in ligaments not all fibers run parallel. Some dense common tissues embrace elastin fibers along with collagen fibers, which allows the ligament to return to its original size after stretching. The ligaments in the vocal folds and between the vertebrae within the vertebral column are sometimes categorised as elastic. This association provides the tissue greater energy in all directions and less power in a single specific path. The dermis of the skin is an instance of dense irregular connective tissue wealthy in collagen fibers. A few distinct cell types and densely packed fibers in a matrix characterize these tissues. In bone, the matrix is inflexible and described as calcified due to the deposited calcium salts. Two main forms of supportive connective tissue, cartilage and bone, permit the physique to keep its posture and shield internal organs. Cartilage the distinctive appearance of cartilage is due to polysaccharides called chondroitin sulfates, which bind with floor substance proteins to form proteoglycans. Embedded within the cartilage matrix are chondrocytes, or cartilage cells, and the space they occupy are known as lacunae (singular = lacuna). A layer of dense irregular connective tissue, the perichondrium, encapsulates the cartilage. Cartilaginous tissue is avascular, thus all vitamins need to diffuse by way of the matrix to reach the chondrocytes. The three main types of cartilage tissue are hyaline cartilage, fibrocartilage, and elastic cartilage. Hyaline Cartilage Hyaline cartilage, the commonest type of cartilage in the body, provides help with some flexibility. The cartilage matrix consists of quick and dispersed collagen fibers and contains massive amounts of proteoglycans. Menisci in the knee joint and the intervertebral discs are examples of fibrocartilage. Tug gently at your ear lobes, and see that the lobes return to their initial shape which is as a result of the external ear incorporates elastic cartilage. Both components of the matrix, organic and inorganic, contribute to the bizarre properties of bone. Bone is a highly vascularized tissue and, unlike cartilage, bone tissue can recuperate from injuries in a relatively short time. They include numerous specialized cells circulating in a watery extracellular matrix containing salts, vitamins, and dissolved proteins. Lymph finally drains into blood vessels, delivering molecules to the blood that would not otherwise immediately enter the bloodstream which incorporates absorbed fat away from the intestine. List and outline the four main tissue varieties Required Materials � None Procedure this activity shall be completed individually or in small groups. Complete the table below by writing the name of the one main tissue sort that greatest applies to every provided description. Identify the most important buildings of the cells in the tissues noticed � nuclei, cell membrane/cilia, extracellular material (fibers and matrix), specialised arrangements of cells Required Materials � Two large items of paper � Drawing utensils Procedure this activity will be accomplished together as a category. Your teacher will direct you to design two totally different epithelial tissues, every of which ought to carry out a selected operate. The functions are: Function Gas Exchange Apical Movement Protection Absorption Description Allows the fast and environment friendly exchange of gases through diffusion from the apical side to the basal aspect of the epithelial sheet Moves supplies across the apical surface of the epithelial sheet. Provides a troublesome barrier between the apical and basal sides of the epithelial sheet to stop the motion of materials. Allows selective trade of enormous supplies through membrane proteins from the apical to the basal side of the epithelial sheet three.
Cheap 7.5 mg mobic visaFibrocartilage plate with a synovia-filled median groove arthritis diet to prevent mobic 15 mg proven, positioned between the articular surfaces made from hyaline cartilage on the proper and left pubic bones arthritis in the knee natural remedies mobic 15 mg order with amex. It is hooked up anteriorly to the intertrochanteric line, posteriorly above to the intertrochanteric crest. A fracture of the neck of the femur can subsequently be intracapsular when in the anterior region or extracapsular when in the posterior region. Strong anterior ligament of the hip joint capsule extending from the ilium to the intertrochanteric line. It radiates into the orbicular zone from the posterior margin of the acetabulum and is also connected to the anterior margin of the higher trochanter and to the intertrochanteric line. Ligament that arises medially from the joint capsule of the pubic bone and extends to the orbicular zone and to the part of the femur proximal to the lesser trochanter. A ring of fibrocartilage and connective tissue that completes and deepens the bony acetabulum. A smooth ligament extending from the acetabular notch to the pit on the head of the femur. Slender extension of fibers from the sacrotuberous ligament to the inner side of the ischium. It passes from the ischial backbone to the sacrum and coccyx and separates the higher from the lesser sciatic foramen. Foramen between the greater sciatic notch, sacrum, sacrospinous ligament and the higher a part of the sacrotuberous ligament. It is traversed by the piriformis muscle, superior and inferior gluteal arteries, veins and nerves, the internal pudendal vein, pudendal nerve, sciatic nerve and posterior femoral cutaneous nerve. Foramen between the lesser sciatic notch and the sacrospinous and sacrotuberous ligaments. It transmits the obturator internus muscle as well as the interior pudendal artery and vein and the pudendal nerve to the ischiorectal fossa. Dorsal mass of ligaments that pass from the tuberosity of the sacrum to the tuberosity of the ilium. Fibrous band originating within the posterior wall of the capsule, extending upward and outward from the tendon of the semimembranous muscle, thereby reinforcing the capsule. Curved band of fibers extending from the epicondyle, across the origin of the popliteal muscle to the head of the fibula, thus reinforcing the posterior wall of the capsule. Aponeurosis from a part of the vastus medialis muscle that extends medially from the patella and attaches to the medial margin of the tibial tuberosity. It maintains the pathway of motion of the patella via muscular contraction and serves as a reserve extension apparatus. Aponeurosis of part of the vastus lateralis lateral to the patella with attachment lateral to the tibial tuberosity. Group of fibers passing anteriorly from the top of the fibula to the tibia, thus holding the two bones together. Weaker group of fibers extending from the posterior part of the head of the fibula to the tibia. It is the field of origin of the lower leg muscles and ensures the steadiness of the malleolar bifurcation. Anterior fibrous bands connecting the fibular incisure to the lateral malleolus, thus stabilizing the malleolar bifurcation. Posterior fibrous bands connecting the fibular incisure to the lateral malleolus, thus stabilizing the malleolar bifurcation. Roughly round ring, the superficial layer of which is made of fibrocartilage, whereas the deep layer is more tendinous. Fibrous band often found connecting the posterior part of sixteen the lateral meniscus with the anterior cruciate ligament. It passes posterior 17 to the lateral meniscus to the fibular floor of the medial femoral condyle behind the posterior cruciate ligament. It passes from the inside surface of the lateral femoral condyle obliquely ahead and inferomedially to the anterior intercondylar area. It prevents inward rotation and ahead displacement of the tibia toward the femur. It passes from the inner floor of the medial femoral condyle to the posterior condylar space, stabilizes the joint when flexed, and prevents backward displacement of the tibia away from the femur. Deformable, paired bulges of the adipose physique that fill empty areas within the anterior part of the joint cavity. Lateral collateral ligament that extends from the lateral epicondyle to the top of the fibula impartial of the capsule and meniscus. Ligament on the medial side of the ankle which consists of the four segments described below. Group of fibers connecting the medial malleolus to the dorsal and medial surfaces of the navicular bone. Segment of the deltoid ligament that connects the medial malleolus to the medial surface of the talus so far as the neck of the talus. Fibers extending posteriorly from the medial malleolus almost so far as the posterior strategy of the talus. It originates in the lateral malleolar fossa and inserts on the lateral tubercle of the posterior process of the talus. It passes obliquely and posteriorly from the apex of the alteral malleolus to the calcaneus. The anterior portion of the lower ankle joint by which the talus articulates with the calcaneus and navicular bones. Joint between the talus and calcaneus that represents the posterior part of the decrease ankle joint. Ligament that passes from the trochlea of the talus to the lateral surface of the calcaneus. Ligament on the medial side of the foot that extends from the medial tubercle of the posterior process of the talus to the sustantaculum tali. The following three interosseous ligaments are present between the tarsal bones: 5 20 Interrosseous talocalcaneal ligament. Joint located in entrance of the talus and calcaneus but proximal to the cuboid and navicular bones. Broad group of ligaments on the dorsum of the foot connecting the navicular bone with the three cuneiform bones. They are particularly important for the bracing of both plantar arches of the foot. It lies medial to the above-mentionend ligament and supports, based on extra traditional view, the articular cavity for the head of the talus. Since the talar aspect of the ligament is type of free and contains no fibrocartilage, this concept is questionable. Groups of ligaments that join the navicular bone with the cuneiform bones lodged in front of it.
Mobic 7.5 mg cheap mastercardExcessive secretion of development hormone in children can result in rheumatoid arthritis medication names buy mobic 7.5 mg lowest price gigantism arthritis herbs mobic 15 mg purchase mastercard, whereas it can lead to in adults if secreted after maturity. Fibular shaft Medial condyle of the tibia the tibial tuberosity is the "bump" below the knee. Medial malleolus Tarsals the distal tibiofibular joint is a fibrous syndesmosis that permits very little movement, growing stability of the low leg. Lateral malleolus Calcaneus Cuboid Fifth metatarsal Middle phalanx First metatarsal Proximal phalanx Distal phalanx A Distal phalanx the soleal line of the tibia marks the attachment of the soleus muscle. Phalanges Medial longitudinal arch Neck of talus Dome of talus the talus articulates with the tibia and fibula superiorly. Metatarsals First proximal phalange First distal phalange the calcaneus and talus bear most of the weight of the physique. A: Lateral view; B: Medial view Bones of the Foot the bones of the foot are organized in a somewhat related trend to the bones of the hand. We have seven tarsals in each foot, a gaggle of three after which a row of four distal to the group of three. The calcaneus has a roughened tuberosity on its plantar facet, the place three muscular tissues originate. The talus is superior to the calcaneus and joins with the distal tibia and distal fibula to kind the ankle joint. A row of four bones lies distal to the calcaneus and the navicular and consists of the medial cuneiform, the center cuneiform, the lateral cuneiform, and the cuboid. The three cuneiforms are regularly called cuneiform 1, 2, and 3, with the first cuneiform all the time the medial one and the third cuneiform at all times the lateral one. The proximal aspect of every metatarsal is called the bottom, and the rounded, distal end of every metatarsal is called a head. The shapes of our foot bones and their relative place to one another trigger the foot to have both longitudinal and transverse arches. We have a longitudinal arch, which runs from the calcaneus to the heads of the metatarsals. The longitudinal arch is often separated right into a medial longitudinal and a lateral longitudinal arch. We also have a transverse arch, which runs medially to laterally across the cuneiforms and cuboid. In addition, ligaments and the intrinsic foot muscular tissues help to preserve our arches. Our arches improve our mobility and balance, and assist in the transfer of weight from one part of the foot to another. Because pes planus can shift gait, it could trigger muscular issues within the leg or thigh. And the trochanteric bursa prevents friction between the larger trochanter and the gluteus maximus muscle. The hip joint permits flexion, extension, abduction, adduction, in addition to inside (medial) and external (lateral) rotation. Knee Joint the knee joint is the articulation between the proximal tibia and distal femur. The rounded condyles of the distal femur match into concave condyles of the proximal tibia. The knee joint is classified as a hinge joint and permits a variety of flexion and extension. The knee joint additionally permits a small amount of medial and lateral rotation, as a outcome of the difference in sizes between the medial and lateral condyles of the femur. The medial condyle of the femur is longer (from front to back) than the lateral condyle of the femur. Thus, as we lengthen our leg toward full extension, the lateral condyles of femur and tibia contact, forming a pivot around which a small quantity of rotation happens. When we convey our knee into full extension, the tibia rotates laterally to cause a perfect fit and "lock" to the knee joint. When flexing our knee from a fully extended position, the tibia must rotate a bit medially to enable flexion to begin. When our weight is on a single leg, and the tibia is thus fixed, the femur rotates laterally to unlock the knee, or the femur rotates medially to "lock" the knee. The giant quadriceps group and the big hamstring muscles provide stability to the joint. Cruciate means "cross," which is an acceptable name, as these two ligaments cross over one another as they pass from the tibia to the femur. The cruciate ligaments stop the femur from sliding off of the tibia anteriorly or posteriorly. The lateral or fibular collateral ligament joins the lateral epicondyle of the femur to the top of the fibula. The medial or tibial collateral ligament joins the medial epicondyle of the femur to the lateral facet of the proximal tibia. The medial collateral ligament is more prone to injury than is the lateral collateral ligament, as a end result of its vulnerability when a pressure pushes into the lateral side of the knee. This ligament runs from the patella to the tibial tuberosity and is a portion of the quadriceps tendon of insertion. The patellar ligament provides further stability throughout the anterior facet of the knee joint. The articulating surfaces of the sacrum and ilium nestle in opposition to one another, in order that the joints permit very little movement. Hip Joint the hip joint is a ball-and-socket joint designed to have the soundness needed for a weight-bearing joint. A robust ring of fibrocartilage, known as the acetabular labrum, connects to the edge of the acetabulum, giving the socket higher depth and serving to to maintain the head of the femur within the socket. The ischiofemoral ligament, the iliofemoral ligament, and the pubofemoral ligament be a part of every of the hip bones to the femur. In addition, the ligament of the top of the femur joins the head of the femur to the acetabulum. The ischial bursa prevents friction between the gluteus maximus muscle and the ischial tuberosity. Pubofemoral ligament the iliolumbar ligament is a half of a posh community of ligaments that stabilize the pelvic girdle and its connection to the lumbar spine. The inguinal ligament is the inferior margin of the aponeurosis of the external oblique muscle and superior border of the femoral triangle. The iliofemoral ligament, shaped like an inverted "Y", helps keep optimum contact between the femoral head and acetabulum, limiting medial rotation and extension of the hip. Anterior sacrococcygeal ligament Obturator membrane Pubic symphysis A the posterior sacroiliac ligaments encompass and stabilize the sacrum. They are half of a large community of thick, robust ligaments situated in the pelvic area. Iliolumbar ligament Sacrospinous ligament Iliofemoral ligament the sacrotuberous ligament stabilizes the sacrum inferiorly and provides muscle attachment points on the posterior pelvis.

15 mg mobic generic with amexThe overzealous investigator could even exacerbate the severity of some situations rheumatoid arthritis definition who generic mobic 15 mg on line, corresponding to persistent idiopathic pain syndromes ease arthritis pain in fingers buy 7.5 mg mobic visa. No substitute exists, nonetheless, for precise medical expertise, and the reader is strongly really helpful to practise the skills of paediatric musculoskeletal examination at each acceptable opportunity. An appreciation of the vary of normality in youngsters and young people is an absolute prerequisite to the detection of abnormality. Most affected children are of their preschool or early school years, and infrequently have issue describing their symptoms. Parents may notice joint swelling if a number of giant peripheral joints are involved, such as the knee (the most typical joint affected), ankle or wrist. It is rarer for youngsters to present with isolated small joint (finger or toe) arthritis or axial joint involvement (such because the shoulder, hip, backbone or temporomandibular joints), and oldsters are additionally less likely to discover swelling in these joints. Diurnal variation of signs, similar to early morning joint stiffness or exacerbation after prolonged relaxation (joint "gelling") are attribute. Joint dysfunction may be manifest by limping, problem with writing or lack of ability to perform different actions of every day residing (Table 15. More aggressive remedy is being utilized in an try to induce early illness remission, an method that has been complemented just lately by a wider therapeutic armamentarium. When the ankle is dorsiflexed, the normally outstanding anterior tendon surface markings could also be obscured by arthritis, though this can be troublesome to see in infants and overweight youngsters. Other relevant observations embody muscle wasting, notably of the vastus medialis and gastrocnemius, and leg length discrepancy, which frequently signifies accelerated development around affected joints. Wrist arthritis could also be finest appreciated by asking the child to press the palms of their palms together within the "prayer" position; a dorsal bulge and decreased vary of motion, especially whether it is asymmetrical, are constant features of synovitis. Swelling of the elbow could be palpated on either aspect of the olecranon and often leads to a flexion deformity of the elbow. Elbow swelling obscures the posterior dimple created when the elbow is fully extended. The small joints of the arms and feet must be inspected and palpated individually; reliable signs of synovitis are the presence of joint margin tenderness, restricted movement, swelling and purplish discoloration, incomplete fist closure and diminished grip strength. Cervical spine involvement could additionally be detected by lack of ability to rotate the head laterally to place the chin on each shoulder and by reduced cervical extension. Temporomandibular synovitis is usually missed; it may prevent full and symmetrical opening of the mouth. Careful statement of gait allows the examiner to evaluate the function of lower limb joints. Children with oligoarthritis are inclined to seem very healthy and have few findings apart from arthritis (most regularly the knee). If asymptomatic continual anterior uveitis has preceded the onset of arthritis, posterior synechiae and/ or band keratopathy could additionally be visible with a hand-held ophthalmoscope targeted on the lens. Differentiating mechanical issues and ache amplification syndromes from arthritis represents one of many best challenges in paediatric rheumatology. The most frequent of these are mechanical disorders similar to hypermobility and trauma, (including non-accidental trauma), followed by infectious and post-infectious illnesses, malignancies, acute and persistent inflammatory disorders and the idiopathic amplification pain syndromes. In younger patients it could be very important contemplate genetic issues of inborn errors of metabolism, and in children with recurrent fevers the auto-inflammatory disorders need to be ruled out. The physical examination demonstrates an additional 10�15 � levels if motion in lax joints. Lower limb findings may be improved by method of custom-moulded semi-rigid insoles with shock-absorbing posts (as indeed could other postural abnormalities of the feet) that goal to assist the longitudinal foot arch and stabilize the ankle. Arthrocentesis has the added advantage, notably within the hip, of lowering intra-articular pressure and minimizing the chance of compromised blood provide to the epiphysis. If the an infection is located near a joint, it could cause a sterile (sympathetic) effusion which may be mistaken for arthritis. Radiographs could also be regular initially or present periosteal reaction; a technetium bone scan helps set up bone infection and stop persistent osteomyelitis. Most mechanical causes of joint pain are inclined to be worse after exercise and because the day goes on, however early morning stiffness the day or two after train may be a characteristic. A subset of sufferers with benign hypermobility complains of dizziness, poor tone and subjective weak point, and some kids with important laxity may indeed have more severe types of Ehlers�Danlos syndrome. Infection-related disorders Reactive arthritis-This is the commonest type of arthritis in childhood. It is characterised by self-limited, acute and painful joint swelling (usually lasting lower than 6 weeks) that follows, or hardly ever accompanies, proof of extra-articular an infection (Box 15. Septic arthritis-Almost completely monoarticular and related to "pseudoparalysis" of the affected limb (extreme ache with the affected joint held rigidly in the place of most comfort). Multi-system inflammatory disease is characteristic, however clinical manifestations are protean. An erythematous, acneiform facial rash could additionally be current, and the basic photosensitive malar rash is a frequent however not a uniform finding. Most kids have hair loss, mouth sores, lymphadenopathy, organomegaly, other rashes and swollen joints. Typical symptoms embrace malaise, progressive proximal muscle weak spot and muscle ache or discomfort. In very weak youngsters, respiratory failure and aspiration pneumonia could additionally be life-threatening. Some youngsters have frank arthritis and infrequently could develop intensive joint limitations that mimic polyarthritis however produce paucity of inflammatory signs, besides morning stiffness. Haematuria is just about always current, and proteinuria may be discovered, however vital renal disease is extraordinarily uncommon. When these youngsters present to the paediatric rheumatologist, their full blood counts are normal, and a high stage of suspicion is required. Early metastases to the bone cause pain that might be troublesome for the doctor to localize. Lymphoma-Lymphoma usually impacts older kids and may present with musculoskeletal symptoms. Idiopathic pain syndromes essentially the most dramatic musculoskeletal ache in children is often discovered in the idiopathic ache syndromes. These could additionally be localized (complex regional ache syndromes) or generalized (diffuse ache syndromes, additionally known as fibromyalgia). Exogenous stress (including college pressures, bullying or other forms of abuse, and even parental pressure) is a standard accompanying function, though usually unrecognized by the mother and father. These kids and adolescents deserve meticulous physical examination and judicious investigation to rule out an underlying organic pathology. Too a lot investigation and vacillating doctor-to-patient communication, nevertheless, could perpetuate or exacerbate the scientific options of those issues.
|