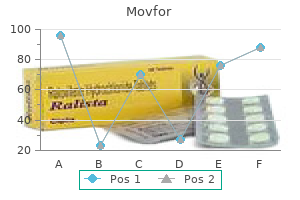
Movfor 200 mg order visaMeasured octanol: buffer partition coefficients and pKa values of clinically used medicine antiviral hiv movfor 200 mg sale. The slim span of axon between these myelinated segments hiv infection rates by continent movfor 200 mg order online, the node of Ranvier, accommodates the ion channels that help action potentials. Probable membrane locations and protein websites for local anesthetics are also proven. Although the membrane is comparatively permeable to potassium ions, an intracellularto-extracellular potassium ratio of a hundred and fifty to 5 mM, or 30:1, is maintained by lively removing of potassium as it leaks passively throughout the plasma membrane into the cell. During an motion potential, the nerve membrane transiently switches its greater permeability from K+ to Na+, thereby changing the membrane potential from negative to optimistic, and again again. Permeation of ions via membranes occurs through specialized proteins known as ion channels. Sodium channels, as nicely as, near an "inactivated" conformation after their preliminary activation. A small membrane depolarization extending along an axon from a region of excited membrane, will start to open each Na+ and K+ channels. After one action potential, the concentrations of Na+ and K+ have changed little for the large myelinated fibers however by as a lot as 10% for the small, nonmyelinated axons. The Na+ ions entering and K+ ions leaving the cell as a result of this course of are restored by the Na+/K+ pump. The precise value of the threshold varies in several regions of the cell and might change with time. Directly after an impulse, when some Na+ channels are nonetheless inactivated and a few K+ channels are nonetheless activated, the edge is above its "resting" worth and the membrane is "refractory" to stimulation. Over time, as Na+ inactivation decays and K+ channels return to their closed conformation, the unique resting threshold value is restored. Positive factors (yellow arrows) improve the speed of depolarization in a positive-feedback loop, with every component within the cycle favoring the following one. Negative elements (gray arrows) lower the depolarization fee by lowering or opposing the associated optimistic issue, with efflux of K+ eventually dominating the ionic move and repolarizing the membrane. When enough of the Na+ channels are blocked, local circuit present fails to deliver the adjoining resting region to threshold, and the impulse is totally extinguished. Therefore as a matter of chemistry (and to optimize shelf life), most of these medicine are formulated as hydrochloride salts. The pKa of the drug and tissue pH decide the quantity of drug that exists in solution as free base or as positively charged cation when injected into residing tissue (see earlier). Furthermore, uptake of the drug by tissue, largely via lipophilic adsorption, may even alter its exercise, each by shifting the effective pKa downward, thereby favoring the impartial base form, and by limiting diffusion of the anesthetic away from the positioning of injection. Moderately hydrophobic local anesthetics block sooner than either hydrophilic or highly hydrophobic ones, delivered on the identical focus, for the next reasons. Moderately hydrophilic local anesthetic block, such as lidocaine, are less certain to tissues than very hydrophobic medicine are. The extremely hydrophobic native anesthetics, having higher intrinsic potencies (see Table 29. Which type of the local anesthetic, charged cation or neutral base, is actually responsible for blockade of impulses More alkaline options of local anesthetics block nerve conduction extra successfully. Modeled from the original research of Hodgkin and Huxley on the squid big axon (see Hodgkin7b), these relationships hold for nearly all invertebrate and vertebrate nerve fibers. Indeed, the local circuit present is so robust that it could skip past two completely nonexcitable nodes. Direct control of axoplasmic pH (or inner perfusion with permanently charged quaternary amine homologs) shows that the dominant potency derives from the cationic species acting from the cytoplasmic surface. The potency of local anesthetics to produce tonic and phasic inhibition is similarly depending on their construction, hydrophobicity, and pKa. There seems to be a single, albeit complex, binding site for local anesthetics on the Na+ channel, with a "tonic" affinity at rest and increased "phasic" affinity occurring on account of depolarization. The sodium channel can be influenced by a quantity of medication or toxins/ venoms, and the completely different websites are numbered. As the focus of local anesthetic applied to the nerve is increased, a decrease within the fee of depolarization and in the peak amplitude of the action potential occurs till the impulse is abolished. When the membrane of isolated neurons is quickly depolarized to a constant worth, the time course of ionic currents is observed. Sodium currents throughout one preliminary depolarization are decreased by subclinical doses of local anesthetic. If the check depolarization is applied repeatedly at frequencies higher than 5 Hz (five pulses per second), the partially depressed (tonically inhibited) Na+ current is further lowered incrementally for each pulse till a brand new steady-state degree of inhibition is reached. Phasic actions are a manifestation of the selective affinity of native anesthetics for conformations of the Na+ channel that outcome from depolarization. Both "open" and "inactivated" states of the channel bind local anesthetics more avidly than the resting state does. Repeated depolarization thus will increase the fraction of drug-bound channels; dissociation of these certain drug molecules is usually a slower process than the conventional recovery from inactivation (see earlier) and results in the use-dependent accumulation of channels in the blocked situation and the phenomenon of phasic block. By its selective binding to a channel state, the native anesthetic stabilizes that state. During phasic block, subsequently, more inactivated channels become drug sure, and reciprocally, much less activation can happen. This relationship between state-dependent affinities and modification of transitions amongst states by way of drug binding is identified as the "modulated receptor" model. Application of the phasic prepare of depolarizations ends in a dynamic discount of currents after every depolarization, with a steady-state value of phasic inhibition reached in the course of the prepare of 75% of management currents. Recovery of currents to the tonic value happens within a quantity of seconds when phasic testing stops (not shown). Stimulation by a train at 20 stimuli per second induces a phasic inhibition that further reduces the amplitude by about 70% from the control worth. As with the ionic currents (A), phasic inhibition of the motion potential recovers quickly when high-frequency stimulation stops. Voltage sensitivity derives from the constructive costs positioned on S4 segments, which slide or swing "outward" in response to membrane depolarization. By linkages still unknown, this motion of S4 leads to a conformational rearrangement of the S6 segments, which form the internal, cytoplasmic entry to the channel. Closed-to-open channel gating results from movement of the S6 segments, whereas inactivation gating outcomes from binding of the cytoplasmic loop situated between D-3 and D-4 to the cytoplasmic opening of the channel. Amino acid mutations in the S6 segments of D-1, D-3, and D-4 all modify native anesthetic action, thus suggesting either that these regions form a "pharmacophore" small enough to simultaneously contact the drug at three surfaces or that the local anesthetic molecule strikes quickly amongst these three segments.
200 mg movfor generic overnight deliveryDisturbances in serum sodium therefore could reflect alterations in glucose metabolism hiv infection rates on the rise movfor 200 mg online buy cheap, renal perform hiv infection on skin discount movfor 200 mg without a prescription, or accumulation of body water. The anesthesiologist is confronted with the query of which levels of electrolytes require therapy earlier than anesthesia. Although slowly developing hyponatremia usually produces few signs, the patient may be lethargic, apathetic, or unbalanced. Chronic hyponatremia is better tolerated than acute hyponatremia due to mechanisms regulating intracellular fluid quantity that alleviate mind edema; the lack of other solutes from cells decreases the osmotic movement of water into cells. By distinction, acute hyponatremia may be manifested by severe signs requiring emergency remedy: profound cerebral edema with obtundation, coma, convulsions, and disordered reflexes and thermoregulatory management. Neither acute nor continual hyponatremia necessitates restoration of serum sodium to normal levels, just till resolution of neurologic symptoms; mind swelling often resolves at a serum sodium level of 130 mEq/L. Because too rapid correction of hypernatremia can result in cerebral edema and probably osmotic demyelination syndrome with convulsions, coma, and demise; correction ought to be made steadily. Hypokalemia and Hyperkalemia Hypokalemia and hyperkalemia are also mentioned in Chapters 31 and 47. The relationship between the measured potassium concentration in serum and total-body potassium shops can finest be described with a scattergram. Only 2% of total-body potassium is saved in plasma (4200 mEq in cells and 60 mEq in extracellular fluid). Thus a 20% to 25% change in potassium levels in plasma may symbolize a change in total-body potassium of a thousand mEq or more if the change had been persistent or as little as 10 to 20 mEq if the change were acute. As with serum sodium levels, acute changes in serum potassium ranges are much less nicely tolerated than persistent adjustments. Chronic modifications are comparatively well tolerated because of the equilibration of serum and intracellular stores that takes place over time to return the resting membrane potential of excitable cells to practically normal levels. Nevertheless, the earliest manifestations of hyperkalemia are narrowing and peaking of the T wave. Although not diagnostic of hyperkalemia, T waves are virtually invariably peaked and slender when serum potassium ranges are 7 to 9 mEq/L. Intravenous administration of bicarbonate, glucose with insulin (1 unit/2 g glucose), can reverse these changes temporarily by shifting extracellular potassium into the cells. Calcium is run to stabilize the cardiac membrane; it has no impact on plasma concentrations of potassium. Furosemide should be given to start the removal strategy of extra potassium from the body and decrease serum potassium levels. Sodium polystyrene sulfonate (Kayexalate) enemas could be given to bind potassium within the gut in change for sodium, these should be used with caution in perioperative sufferers as there are reports of intestinal necrosis. Indeed, the plasma potassium focus measured in samples instantly earlier than surgical procedures is normally 0. A -adrenergic receptor stimulating agent (20 mg of nebulized albuterol for a 70-kg patient) can be utilized to deal with hyperkalemia when it happens; it decreases potassium ranges 1. In a hyperkalemic patient, hypoventilation can be dangerous throughout anesthesia as a result of each zero. As with hyperkalemia, information of the cause of the potassium deficiency and applicable preoperative evaluation and treatment of that cause could additionally be as important as therapy of the deficiency itself. Also like hyperkalemia, hypokalemia may replicate small or huge modifications in total-body potassium. The major worrisome manifestations of hypokalemia pertain to the circulatory system, both the cardiac and peripheral components. In addition, continual hypokalemia ends in muscle weak spot, hypoperistalsis, and nephropathy. Cardiovascular manifestations of hypokalemia embody the next: autonomic neuropathy, orthostatic hypotension, decreased sympathetic reserve, impaired myocardial contractility, and electrical conduction abnormalities. Conduction abnormalities can current as sinus tachycardia, atrial and ventricular arrhythmias, and intraventricular conduction disturbances that may progress to ventricular fibrillation. Surawicz found these adjustments to be invariably current when serum potassium ranges decreased to less than 2. Replenishing the total-body potassium deficit for a depletion reflected by a serum deficit of 1 mEq/L. Potassiumdepleted myocardium is unusually delicate to digoxin, calcium, and most important, potassium. Rapid potassium infusion in a hypokalemic affected person can produce arrhythmias as severe as those produced by hypokalemia itself, again, sluggish correction is preferred. The urgency of the operation, the degree of electrolyte abnormality, the medicines given, the acid-base stability, and the suddenness or persistence of the electrolyte disturbance are all concerns. For example, a small study of sufferers undergoing vascular entry procedures with preoperative potassium levels of higher than 6 mmol/L demonstrated no antagonistic outcomes. Of these 1910 sufferers, hyperkalemia contributed to death in 7, and the incidence of issues of potassium remedy was 1 in 250. Potassium repletion decreased the number of ectopic ventricular beats per affected person from seventy one. Preoperative preparation ought to embrace knowledge of disease processes and their effects to information the patient easily via the perioperative period. These results could benefit fast induction of anesthesia with the applying of cricoid strain or endotracheal intubation with the patient unanesthetized (awake), preoperative nasogastric suctioning, or preoperative use of histamine receptor blocking medicine. This lower may be attributable to the use of higher technique, extra acceptable prophylactic timing and use of antibiotics, better vitamin, less invasive (laparoscopic and endoscopic) surgery, upkeep of normothermia, and surgical resection of even tumors. For example, they might be anemic from deficiencies in iron, intrinsic factor, folate, or vitamin B12. Respiration could additionally be impaired because of tobacco abuse, peritonitis, abscess, pulmonary obstruction, earlier incisions, aspiration, or pulmonary embolism (as occurs with ulcerative colitis or with thrombophlebitis in bedridden patients). These patients may also have hepatitis, cholangitis, unwanted effects from antibiotic medicine or other medications, large bleeding with anemia and shock, or psychological derangements. Ulcerative Colitis and Carcinoid Tumors as Examples of Gastrointestinal Disease Affecting Other Systems Ulcerative colitis is a persistent inflammatory disease of the colonic mucosa, typically starting within the rectum and lengthening proximally by way of the colon. It is often marked with an unpredictable clinical course with durations of remission and exacerbation. Patients with ulcerative colitis can also have the following: phlebitis; deficiencies in iron, folate, or vitamin B12; anemia; or clotting issues brought on by malabsorption. They can current as malnourished or dehydrated, or with electrolyte abnormalities. In addition, ulcerative colitis can be accompanied by massive bleeding, bowel obstruction, bowel perforation, toxic megacolon, hepatitis, arthritis, iritis, spondylitis, diabetes, or pancreatitis. Cardiac involvement, although frequently reported, is usually limited to right-sided valvular and myocardial plaque formation. Some do, however, and surprising carcinoid can manifest intraoperatively by hypersecretion of gastric fluid.
200 mg movfor discount with amexMechanism for bupivacaine despair of cardiac conduction: quick block of sodium channels in the course of the action potential with sluggish restoration from block throughout diastole young living antiviral 200 mg movfor otc. Inhibition of calcium-induced calcium release from purified cardiac sarcoplasmic reticulum vesicles anti viral hand wipes movfor 200 mg discount on-line. Comparison of the effects of bupivacaine and ropivacaine on coronary heart cell mitochondrial bioenergetics. The Third American Society of Regional Anesthesia and Pain Medicine apply advisory on local anesthetic systemic toxicity: government summary 2017. Validity of the lipid sink as a mechanism for the reversal of native anesthetic systemic toxicity: a physiologically based mostly pharmacokinetic mannequin research. Pretreatment or resuscitation with a lipid infusion shifts the dose-response to bupivacaine-induced asystole in rats. Treatment of acute systemic toxicity after the speedy intravenous injection of ropivacaine and bupivacaine within the acutely aware dog. Influence of lidocaine and bupivacaine on isolated guinea pig atria within the presence of acidosis and hypoxia. Injuries associated with regional anesthesia within the Nineteen Eighties and Nineties: a closed claims analysis. Irreversible conduction block in isolated nerve by high concentrations of native anesthetics. Transient neurologic symptoms after spinal anesthesia: an epidemiologic research of 1,863 sufferers. A quantitative systematic overview (meta-analysis) of randomized controlled studies]. Systemic morphine enhances unfold of sensory analgesia throughout postoperative epidural bupivacaine infusion. Pharmacokinetic nature of tachyphylaxis to lidocaine: peripheral nerve blocks and infiltration anesthesia in rats. Effect of previous scorpion bite(s) on the motion of intrathecal bupivacaine: a case management study. Effects of epinephrine in native anesthetics on the central and peripheral nervous systems: neurotoxicity and neural blood move. Effect of procaine, carbocain and xylocaine on cutaneous muscle in rabbits and mice. Tricyclic antidepressants and their native anesthetic properties: from bench to bedside and back again. Techniques for periarticular infiltration with liposomal bupivacaine for the administration of pain after hip and knee arthroplasty: a consensus advice. Liposomal bupivacaine as a single-injection peripheral nerve block: a doseresponse examine. A phase 1, dose-escalation, double-blind, block-randomized, controlled trial of security and efficacy of neosaxitoxin alone and in combination with zero. Anesthesia-related (and surgery-related) danger is usually defined as morbidity and mortality occurring inside 30 days of surgery, though events that occur at later factors should be related to anesthesia and/or surgery. In the literature on anesthesia-related risk, the rates of morbidity and mortality reported throughout research show a considerable variability partly attributable to the broad range of definitions used in these studies. Historical research of anesthesia-related danger identified anesthesia-related respiratory depression as the main cause of death and coma totally attributable to anesthesia. Research into anesthesia-related cardiac arrest has found it to be attributable to treatment administration, airway administration, and technical issues of central venous access. Multivariate modeling can be utilized to determine specific components related to an elevated chance of antagonistic postoperative events, and it has been used to outline a range of medical danger indices to predict postoperative outcomes. Surveys of maternal mortality recommend that though the absolute rate of complications attributable to anesthesia has not decreased over time, the elevated use of regional anesthesia might have led to enhancements in end result. Growth within the number and variety of surgical procedures performed in hospital outpatient departments, ambulatory surgical procedure facilities, and doctor workplaces creates novel challenges for assessing and managing perioperative threat. Emerging evidence suggests that the choice of anesthetic medicine, ventilator methods, or technique could influence patient outcomes. Introduction Since the start of its trendy history, the administration of anesthesia has been acknowledged as a hazardous enterprise,1 with distinct dangers to the patient and occupational risks to anesthesia suppliers. From the attitude of public health, understanding both the character and the magnitude of these risks is necessary on a number of ranges. For particular person patients, receiving accurate information on the chance of specific perioperative issues is a prerequisite for informed decision making related to anesthesia and surgery. More broadly, understanding the extent to which rates of perioperative morbidity and mortality 892 vary across sufferers, physicians, and hospitals supplies an essential opportunity for assessing and improving high quality in healthcare. Efforts to decide the dangers of anesthesia are complicated by many potential perspectives from which such risks could be defined. The use of alternate durations of remark for morbidity and mortality-the intraoperative period alone, the primary 48 hours after surgery, the length of the hospital stay, or the primary 30 days or longer after surgery- complicates easy conclusions concerning the risks confronted by any particular person patient present process anesthesia and surgery and at what point after surgery the probability of additional adverse occasions has returned to baseline (Table 30. Studies solely focusing on the intraoperative interval have characterized contemporary anesthesia care as a patient security "success story" because of the low charges of dying instantly attributable to anesthesia care. As a outcome, anesthesia has been hailed by the National Academy of Medicine as "an area during which very spectacular improvements have been made" when it comes to affected person safety. In this case, the decision to view the perioperative infarction primarily as a consequence of patient illness or as an occasion that could be prevented by anesthesia care carries vastly different implications for efforts to define and scale back the dangers of anesthesia. Finally, the diverse array of outcomes considered as hazards of anesthesia complicate the interpretation of the literature on the dangers of anesthesia. Traditionally, investigators have focused on issues of dying and main morbidity similar to myocardial infarction, pneumonia, and renal failure. More just lately, nevertheless, this view has been broadened to embody economic outcomes, as nicely as patient-centered outcomes such as useful independence, high quality of life, and satisfaction (Table 30. In this text, current theories concerning the underlying causes of antagonistic occasions within the perioperative period are reviewed, and the historical and contemporary literature concerning the nature and magnitude of risk related to both intraoperative anesthesia care and perioperative care are examined. Next, historical and recent efforts to characterize the patient-, provider-, and facility-level determinants of anesthetic and perioperative danger are reviewed through statistical risk indices, and clinically based mostly approaches to affected person classification, and obtainable literature on the determinants of threat unique to the obstetric, pediatric, and geriatric populations are mentioned. Finally, future directions in research and scientific care associated to anesthetic danger are discussed, with a give attention to the well being coverage implications of adjusting knowledge relating to the hazards of anesthesia. With respect to anesthesia, the selection and effects of medicines, including risky and intravenous anesthetic medicine, and the talents of the practitioner are important. Further, practitioners could affect outcomes at multiple points within the postoperative course. Anesthesia-related contributions can include problems with judgment and mishaps, in addition to traits of the provider. The surgical process itself affects outcome, as does the location of intraoperative and postoperative care. Given these challenges and opportunities, the objective of the subsequent section is to summarize the present state of knowledge on this space, including the relative strengths and weaknesses of randomized and nonrandomized. For research of perioperative mortality, particular person instances could be reviewed to decide the cause of mortality. Alternatively, data on all patients within the cohort examine can be obtained, and discrete components associated with the event of morbidity or mortality can be decided, often utilizing multivariate regression strategies. An instance of a prospective cohort examine to establish elements associated with perioperative cardiac morbidity and mortality is that of Goldman and colleagues,13 which led to development of the Cardiac Risk Index.
200 mg movfor cheap mastercardWithin 6 to 8 hours of withdrawal hiv infection australia movfor 200 mg buy low cost, the affected person might become tremulous antiviral home remedy purchase movfor 200 mg amex, a state that usually subsides inside days or perhaps weeks. Alcoholic hallucinosis and withdrawal seizures usually happen inside 24 to 36 hours. These seizures are generalized grand mal attacks; when focal seizures occur, different causes should be sought. Delirium tremens normally seems within 72 hours of withdrawal and is usually preceded by tremulousness, hallucinations, or seizures. These three symptoms, combined with perceptual distortions, insomnia, psychomotor disturbances, autonomic hyperactivity, and, in a large proportion of circumstances, another potentially fatal sickness. Nutritional problems of alcoholism embrace alcoholic hypoglycemia and hypothermia, alcoholic polyneuropathy, Wernicke-Korsakoff syndrome, and cerebellar degeneration. In addition, approximately 20% of sufferers with alcoholism also have respiratory disease. Further, postoperatively these sufferers can have poor wound healing, altering levels of consciousness/delirium, and problem with analgesia. Uremic polyneuropathy is a distal symmetric sensorimotor polyneuropathy that might be improved by dialysis. The use of depolarizing muscle relaxants in patients with polyneuropathies has been questioned. Pernicious anemia caused by vitamin B12 deficiency may end in subacute combined degeneration of the spinal wire; the signs are similar to these of continual nitrous oxide toxicity. Both pernicious anemia and nitrous oxide toxicity are related to peripheral neuropathy and issues of the pyramidal tract and posterior column (which governs fine motor skills and the sense of physique position). Combined-system illness can even happen with out anemia, as can nitrous oxide toxicity in dentists and nitrous oxide abusers. Patients with vitamin B12 deficiency and anemia, if handled with folate, enhance hematologically but progress to dementia and severe neuropathy. It may thus be prudent to give an intramuscular injection of a hundred g of vitamin B12 or 800 g orally earlier than giving folate to a affected person who has signs of combined-system degeneration. Drugs utilized in anesthetic management which are reported to be secure for patients with porphyria embody neostigmine, atropine, succinylcholine, nitrous oxide, procaine, propofol, etomidate, meperidine, fentanyl, morphine, droperidol, promazine, promethazine, and chlorpromazine. Propofol has been used with out provoking porphyria in at least two susceptible sufferers. Neuropathies may contain all components of the nerve, thereby producing sensory, motor, and autonomic dysfunction, or just one component. Myasthenia gravis is a disorder of the muscular system brought on by partial blockade or destruction of nicotinic acetylcholine receptors by IgG antibodies. The severity of the illness correlates with the ability of antibodies to decrease the variety of available acetylcholine receptors. For that cause, all anticholinergic medicine could additionally be withheld for six hours preoperatively, and drugs must be reinstituted postoperatively with excessive caution because the sensitivity of these patients to such medication may have modified. Small doses of succinylcholine can be used to facilitate endotracheal intubation; extraordinarily small doses of nondepolarizing medication can be utilized for intraoperative rest not achieved by regional anesthesia or risky anesthetics. Of prime importance is monitoring neuromuscular blockade because the guide for muscle relaxant administration and their reversal. Previously, controlled mechanical air flow was frequently required for 24 to forty eight hours postoperatively; nevertheless, quick extubation has become more widespread. Another study found that epidural analgesia intraand postoperatively decreased the requirement of mechanical ventilation following thymectomy, though this was retrospective in nature. Lambert-Eaton syndrome (myasthenic syndrome) is characterised by proximal limb muscle weakness and is related to antibodies directed against the voltagegated calcium channels in presynaptic nerve terminals. Strength or reflexes sometimes improve with repetitive effort, as affected sufferers exhibit decreased release of acetylcholine at the neuromuscular junction and repetitive use will increase the out there junctional acetylcholine. Guanidine remedy enhances the release of acetylcholine from nerve terminals and improves power. Men with this syndrome usually have small cell carcinoma of the lung or other malignant disease, whereas girls usually have malignant illness, sarcoidosis, thyroiditis, or a collagen-related vascular illness. In addition, these patients have elevated sensitivity to both depolarizing and nondepolarizing muscle relaxants. Dermatomyositis and polymyositis are characterized by proximal limb muscle weak point with dysphagia. These circumstances are associated with malignant illness or collagen-related vascular illness and infrequently involve respiratory and cardiac muscle. Periodic paralysis is one other disease in which sensitivity to muscle relaxants will increase. Periodic weak spot begins in childhood or adolescence and is precipitated by rest after exercise, sleep, chilly, surgical procedure, or pregnancy. Hypokalemic and hyperkalemic forms exist and are related to cardiac arrhythmias. Like thyrotoxic periodic paralysis, these hypokalemic and hyperkalemic varieties usually spare the respiratory muscles. Anesthetic management consists of minimizing stress, maintaining normal fluid and electrolyte standing, and controlling physique temperature. As with the opposite types of muscular dystrophy, most problems in myotonic dystrophy come up from cardiac arrhythmias and inadequacy of the respiratory muscle tissue. Volatile anesthetics are associated with anesthesia-induced rhabdomyolysis, hyperkalemia, and cardiac arrest; due to this fact, whole intravenous anesthesia is the popular method of general anesthesia. Prophylaxis with intravenous dantrolene sodium may also be warranted with high risk patients. Malignant hyperthermia happens most incessantly in youngsters and adolescents; the incidence is 1 in 14,000 administrations of anesthesia. Patients with these indicators, giant ventricles (as seen on radiography or pictures of the brain), or edema surrounding supratentorial tumors should be considered at risk for intraoperative intracranial hypertension. These sufferers could profit from preoperative therapy or anesthetic management that assumes this chance. Renal Disease and Electrolyte Disorders the anesthesiologist has an necessary function to play in preventing the onset and consequences of renal failure and its initiators. The linking of renal failure to electrolyte issues is extra apparent: the kidney is the first organ for regulating physique osmolality and fluid quantity and has a serious position in excretion of the top products of metabolism. In performing these features, the kidney becomes intimately involved in the excretion of electrolytes. A affected person with renal insufficiency whose personal kidneys are still functioning is distinct not only from a patient with end-stage renal illness whose renal features are offered by dialysis but additionally from a patient who has a transplanted kidney. In addition, acute adjustments in renal perform present fairly a different drawback than do chronic alterations in operate. Certain renal diseases require different preoperative preparation than others, however generally, renal illness of any origin presents the identical preoperative issues. It is related to congenital cardiac lesions such as endocardial cushion defects (40%), ventricular septal defects (27%), patent ductus arteriosus (12%), and tetralogy of Fallot (8%).
Diseases - Johnson Munson syndrome
- Wright Dick syndrome
- Epilepsy benign neonatal familial 2
- Chromosome 21, monosomy 21q22
- Progressive hearing loss stapes fixation
- Lobar atrophy of brain
- Gymnophobia
- Deafness hyperuricemia neurologic ataxia
- Letterer Siwe disease
Buy movfor 200 mg visaProbiotics and synbiotics for the prevention of postoperative infections following belly surgery: a scientific review and meta-analysis of randomized controlled trials hiv infection rate in sierra leone cheap movfor 200 mg with visa. Prevention of necrotizing enterocolitis with probiotics: a scientific review and meta-analysis highest hiv infection rate by country generic 200 mg movfor visa. Differential analysis of sleep disorders, non-epileptic attacks and epileptic attacks. Treatment of standing epilepticus: a prospective comparability of diazepam and phenytoin versus phenobarbital and optional phenytoin. Rigidity and pulmonary edema after Innovar in a patient on levodopa therapy: report of a case. Frequency and traits of silent dementia among elderly Japanese-American males: the Honolulu-Asia Aging Study. The common inhalational anesthetic isoflurane induces apoptosis via activation of inositol 1,4,5-trisphosphate receptors. The inhalation anesthetic desflurane induces caspase activation and increases amyloid beta-protein ranges beneath hypoxic circumstances. The long-term medical outcomes of Lyme disease: a population-based retrospective cohort examine. Anesthetic administration for surgical corrections of severe flexion deformity of the cervical backbone. Repeated spinal anesthesia in a tetraparetic patient with Guillain-Barr� syndrome. Plasmapheresis and Guillain-Barr� syndrome: analysis of prognostic factors and the impact of plasmapheresis. Effect of prethymectomy plasma change on postoperative respiratory perform in myasthenia gravis. Predicting the need for postoperative mechanical ventilation in myasthenia gravis. Criteria for postoperative mechanical air flow after thymectomy in patients with myasthenia gravis: a retrospective analysis. Anesthesia for unsuspected Lambert-Eaton myasthenic syndrome with autoantibodies and occult small cell lung carcinoma. Successful anesthetic administration of a affected person with hypokalemic familial periodic paralysis present process cardiac surgical procedure. Atlantoaxial instability in people with Down syndrome: epidemiologic, radiographic, and medical studies. Intracranial hypertension throughout surgery for supratentorial tumor: correlation with preoperative computed tomography scans. Pathophysiology and prevention of acute renal failure: the position of the anaesthetist. A multicenter, randomized, managed scientific trial of transfusion necessities in important care: Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. Persistant effect of red cell transfusion on health-related quality of life after cardiac surgery. Perioperative anesthesia clinical trials g: restrictive or liberal red-cell transfusion for cardiac surgical procedure. Renal dysfunction after myocardial revascularization: danger factors, adverse outcomes, and hospital useful resource utilization. Evaluation of induction doses of propofol: comparability between endstage renal disease and regular renal function patients. Patterns of therapy and correction of hyponatremia in intensive care unit patients. Asymptomatic cecal perforation in a renal transplant recipient after sodium polystyrene sulfonate administration. Small intestinal transplant mucosal necrosis related to enteral sodium polystyrene sulfonate administration. Hypokalemia before induction of anesthesia and prevention by beta2 adrenoceptor antagonism. Acute intravenous administration of potassium chloride to furosemide pretreated dogs. Preoperative serum potassium ranges and perioperative outcomes in cardiac surgical procedure patients: multicenter Study of Perioperative Ischemia Research Group. Diuretics, serum potassium and ventricular arrhythmias in the a quantity of risk issue intervention. Ulcerative colitis practice pointers in adults: American College of Gastroenterology, Practice Parameters Committee. Perioperative normothermia to reduce the incidence of surgical-wound infection and shorten hospitalization: examine of Wound Infection and Temperature Group. Anesthetic administration of patients with carcinoid syndrome and carcinoid coronary heart disease: the Mount Sinai algorithm. Review of the anaesthetic administration of 21 sufferers present process laparotomy for carcinoid syndrome. Intraoperative administration of patients with carcinoid heart illness having valvular surgical procedure: a evaluation of one hundred consecutive cases. Carcinoid crisis throughout anesthesia: profitable remedy with a somatostatin analogue. The prophylactic use of octreotide in a affected person with ovarian carcinoid and valvular coronary heart disease. Octreotide-induced bradycardia and coronary heart block throughout surgical resection of a carcinoid tumor. Psychosocial factors within the irritable bowel syndrome: a multivariate examine of patients and non-patients with irritable bowel syndrome. A comparison of conservative and aggressive transfusion regimens within the perioperative management of sickle cell disease. Primary position for adherent leukocytes in sickle cell vascular occlusion: a model new paradigm. Intraoperative death throughout caesarean section in a affected person with sickle-cell trait. Pro: change transfusion is required for sickle cell trait patients present process cardiopulmonary bypass. Assessment of the use of transfusion therapy perioperatively in patients with sickle cell hemoglobinopathies. Controlled trial of transfusions for silent cerebral infarcts in sickle cell anemia. Perioperative transfusion administration in patients with sickle cell anaemia present process a total hip arthroplasty: is there a role of red-cell change transfusion Anesthesia utilizing plasmapheresis and compelled air warming in a affected person with extreme cold agglutinin hemolytic anemia. Increased preoperative collection of autologous blood with recombinant human erythropoietin remedy. A randomized medical trial of granulocyte transfusion for infection in acute leukemia.
200 mg movfor generic with amexTo achieve an effective goal concentration hiv infection timeline discount movfor 200 mg on line, the conventional teaching of administering an initial dose as calculated by the product of target concentration and volume of distribution countries with high hiv infection rates order movfor 200 mg without a prescription, followed by a upkeep price as calculated because the product of goal concentration and clearance, is inaccurate. The preliminary dose could additionally be calculated because the product of goal concentration and quantity of distribution at peak impact. Maintenance charges must initially account for the distribution of drug in peripheral tissues and may solely be lowered to the product of target focus and clearance after equilibration of plasma and peripheral tissue concentrations. The context-sensitive decrement time is the time for a given decrement in drug concentration, as a operate of the length of infusion that maintains a gentle plasma focus. Contextsensitive decrement instances correctly incorporate the multicompartment behavior of intravenous anesthetics. Alfentanil, fentanyl, sufentanil, remifentanil, propofol, thiopental, methohexital, etomidate, ketamine, midazolam, and dexmedetomidine can all be administered as a steady intravenous infusion. Specific caveats, infusion charges, and titration guidelines are presented in this textual content. Although these methods have typically performed well clinically, they remain beneath investigation. In 1628, William Harvey proved in Exercitatio Anatomica de Motu Cordis et Sanguinis in Animalibus that venous blood was transported to the arterial circulation and thus to physique organs by the center. That drugs injected into veins might be quickly carried to the whole body was rapidly recognized. Consequently, for intravenous drug supply to be successful, predictable intravenous access is crucial. The growth of intravenous methods of anesthetic drug supply has been made attainable by technologic advances. In the middle of the seventeenth century, Christopher Wren and his Oxford contemporaries applied a feather quill and animal bladder to inject medicine into canines and humans and rendered them unconscious. Contemporary needles, catheters, and syringes are descendants of these early devices. In the twentieth century, equipment started to be manufactured from plastics, first polyvinyl chloride, then Teflon, and later, polyurethane. Maintenance of anesthesia by intravenously administered anesthetics has become practical, protected, and well-liked up to now 2 a long time. The discovery of propofol in 1977 supplied the anesthetic apply an intravenous drug appropriate for both induction and upkeep of anesthesia; at present, propofol continues to be some of the incessantly used medication for this function. In addition, a few of the nondepolarizing neuromuscular blocking brokers are used as steady infusions in particular situations. Drugs are nonetheless predominantly injected as a bolus or continuous infusion utilizing standard dosing guidelines, thereby ignoring the large interindividual variability in the dose-response relationship. Therefore manually adjusting the intravenous drug injection regimens to keep an internet measured plasma focus is inconceivable. It turns into much more advanced if a specific effect-site concentration is the target. Optimal patient-individual dosing could additionally be achieved by the appliance of pharmacokinetic-pharmacodynamic principles. Additionally, recent findings recommend that the pharmacokinetic and pharmacodynamic interactions throughout intravenous administration of assorted drugs are necessary and, as such, ought to be taken under consideration when optimizing drug administration. Closed-loop management of drug administration utilizing the scientific measure is indicated as suggestions control. A more recent technologic improvement in intravenous anesthesia is the introduction of computerized pharmacokinetic model�driven continuous-infusion units, enabling the attainment of desired plasma ranges of an intravenous anesthetic drug through the use of a computercontrolled infusion pump operated in accordance with the printed pharmacokinetics of the drug. Systems have been developed for closed-loop administration of various medication similar to neuromuscular blocking agents, hypnotics, and opioids. The control variables for these systems have included various pharmacodynamic measures derived from strategies corresponding to acceleromyography, automated blood stress measurement, and electroencephalography. Before reviewing delivery strategies and devices for intravenous anesthesia, this chapter presents some pharmacokinetic and pharmacodynamic ideas as background for understanding tips on how to administer intravenous drugs to their best benefit. Further discussion of the rules of pharmacokinetics and pharmacodynamics can be present in Chapter 23. Pharmacokinetic Considerations the purpose of optimum intravenous drug dosing is to attain and maintain a desired time course of therapeutic drug effect as accurately as possible, thereby stopping doserelated antagonistic drug results. To be useful in anesthesia, this time course ought to include a fast onset of clinical effects, easy maintenance, and quick restoration after the termination of drug administration. The pharmacokinetics of many intravenous medicine may be described utilizing mammillary multicompartment pharmacokinetic fashions. These models assume that the drug is instantly given and combined within the plasma, leading to a direct peak in its plasma focus. Unfortunately, when one single bolus is used, the preliminary dose should be large sufficient to preserve a focus above the bottom therapeutic focus even at the finish of surgical procedure. However, this generally very giant dose of drug may cause quite a few side effects attributable to the initially high concentrations within the physique. It might be less harmful to keep the drug concentration above the lowest therapeutic level with out very excessive initial concentrations by repeatedly injecting smaller doses; even with this technique, nonetheless, maintaining a steady plasma focus remains to be impossible. To produce a time course of drug effect that follows the time course of anesthetic requirement, a continuous infusion titrated to the perceived anesthetic requirement should be used. Typically, simply enough amount of drug is given to achieve the therapeutic blood or plasma drug focus. Drug administration thereafter ought to be continuously titrated all through surgical procedure. Therefore a mixture of an preliminary bolus adopted by a stepwise reducing steady infusion is more useful. In this article, an evidence of how pharmacokinetic models can be utilized to calculate correct dosing schemes for use with intravenous drug delivery techniques is offered. Pharmacokinetic fashions are mathematical descriptions of how the physique disposes of drugs. The parameters describing this course of are estimated by administering a identified dose of the drug and measuring the ensuing plasma concentrations. A mathematical model then relates the input over time, I(t), with the concentrations over time, C(t). Drug concentrations constantly decrease after the bolus, and the rate of decrease is approximately proportional to the quantity of drug in plasma. The curve might need a single exponent, during which case the plasma concentrations over time might be described by the function C(t) = Ae-kt, the place A is the focus at time 0 and k is a continuing that describes the rate of decrease in concentration. The relationship appears to be a straight line when graphed because the log of focus versus time. A extra common approach to consider pharmacokinetics is to decompose the enter into a collection of small bits (boluses) and think about each little bit of drug individually. The common pharmacokinetic model of drug disposition commonly used in anesthesia independently considers each little bit of drug and analyzes its contribution by the use of polyexponential decay over time. The formal mathematic description of each little bit of drug by method of polyexponential decay over time is the relationship (Eq.
Generic movfor 200 mg mastercardRisks of cardiovascular adverse occasions and demise in patients with previous stroke undergoing emergency noncardiac hiv infection wbc count movfor 200 mg order with mastercard, nonintracranial surgical procedure: the importance of operative timing hiv infection vaccine order 200 mg movfor with visa. The preoperative cerebrovascular session: frequent cerebrovascular questions before basic or cardiac surgery. Atlantoaxial subluxation in several intraoperative head positions in patients with rheumatoid arthritis. American College of Rheumatology 2008 suggestions for the usage of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis. Perianaesthetic dangers and outcomes of belly surgery for metastatic carcinoid tumours. Should dosing of rocuronium in overweight sufferers be based mostly on ideal or corrected body weight. Kostopanagiotou G, Smyrniotis V, Arkadopoulos N, Contis J, Briassoulis G, Kostopanagiotou E. Anaesthetic and perioperative administration of paediatric organ recipients in nontransplant surgical procedure. Anaesthesia for patients with idiopathic environmental intolerance and persistent fatigue syndrome. A critical evaluate of studies evaluating the connection of mode of delivery to perinatal transmission of human immunodeficiency virus. Predictors of operative consequence in sufferers with human immunodeficiency virus an infection and purchased immunodeficiency syndrome. Anesthesia and analgesia in addicts: foundation for establishing a normal working process. Preoperative alcohol screening scores: association with issues in males present process whole joint arthroplasty. Preoperative alcohol consumption and postoperative complications: a scientific evaluate and meta-analysis. Use of the screening advised by the National Institute on Alcohol Abuse and Alcoholism and of a newly derived tool for the detection of unhealthy alcohol drinkers amongst surgical sufferers. Improving the detection of illicit substance use in preoperative anesthesiological assessment. Utility of cocaine drug screens to predict secure delivery of common anesthesia for elective surgical sufferers. The patient recovering from alcohol or drug addiction: particular issues for the anesthesiologist. Ethical Guidelines for the Anesthesia Care of Patients With Do-Not-Resuscitate Orders or Other Directives That Limit Treatment; 2013. A randomized, managed trial of advanced care planning discussions during preoperative evaluations. Preoperative laboratory testing in patients present process elective, low-risk ambulatory surgery. Effectiveness of non-cardiac preoperative testing in non-cardiac elective surgery: a scientific review. Preoperative laboratory investigations: charges and variability previous to low-risk surgical procedures. Preoperative screening for sickle cell illness in youngsters: clinical implications. Effectiveness of preoperative screening for sickle cell illness in a References 998. Operations on sufferers deemed "unfit for operation and anaesthesia": what are the implications Reliability of the American Society of Anesthesiologists bodily standing scale in medical practice. Development and validation of a danger quantification index for 30-day postoperative mortality and morbidity in noncardiac surgical sufferers. Postoperative mortality in the Netherlands: a population-based evaluation of surgery-specific risk in adults. The Surgical Mortality Probability Model: derivation and validation of a easy threat prediction rule for noncardiac surgery. Inpatient hospital admission and death after outpatient surgery in elderly sufferers: significance of patient and system traits and location of care. The Society of Thoracic Surgeons 2018 adult cardiac surgical procedure threat fashions: half 1-background, design considerations, and mannequin improvement. Risk stratification instruments for predicting morbidity and mortality in grownup patients undergoing main surgical procedure: qualitative systematic evaluation. The Surgical Risk Scale as an improved software for risk-adjusted analysis in comparative surgical audit. Focused transthoracic echocardiography predicts perioperative cardiovascular morbidity. Focused echocardiography: a systematic review of diagnostic and clinical decision-making in anaesthesia and important care. A systematic evaluate of the function of cardiopulmonary train testing in vascular surgical procedure. Do selective cyclo-oxygenase-2 inhibitors and conventional non-steroidal anti-inflammatory medicine enhance the chance of atherothrombosis Association of selective serotonin reuptake inhibitors with transfusion in surgical sufferers. Validation of the transient pain inventory in sufferers six months after cardiac surgical procedure. Preoperative nervousness and concern: a comparability of assessments by sufferers and anesthesia and surgery residents. The Toronto General Hospital Transitional Pain Service: development and implementation of a multidisciplinary program to forestall persistent postsurgical ache. Efficacy and financial good factor about an anesthesiologist-directed university preadmission analysis center. A survey on the meant purposes and perceived utility of preoperative cardiology consultations. Use of outpatient preoperative analysis to decrease length of keep for vascular surgery. Alpha-2 adrenergic agonists for the prevention of cardiac complications amongst sufferers present process surgical procedure. Preoperative analysis clinic go to is related to decreased threat of in-hospital postoperative mortality. Development of a preoperative affected person clearance and session screening questionnaire. Comanagement of hospitalized surgical sufferers by drugs physicians in the United States. Orthogeriatric care fashions and outcomes in hip fracture patients: a systematic review and metaanalysis. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial.
200 mg movfor discount mastercardComparison of the prognostic accuracy of scoring systems hiv infection rates by continent movfor 200 mg buy low price, cardiopulmonary exercise testing hiv infection rates heterosexual vs homosexual buy 200 mg movfor mastercard, and plasma biomarkers: a single-centre observational pilot examine. The prognostic worth of pre-operative and post-operative B-type natriuretic peptides in sufferers undergoing noncardiac surgical procedure: B-type natriuretic peptide and N-terminal fragment of pro-B-type natriuretic peptide: a systematic review and particular person affected person data meta-analysis. Randomized comparability of sevoflurane versus propofol to reduce perioperative myocardial ischemia in patients present process noncardiac surgery. Association of troponin T detected with a extremely delicate assay and cardiac construction and mortality threat in the common inhabitants. Association of serial measures of cardiac troponin T using a delicate assay with incident coronary heart failure and cardiovascular mortality in older adults. High sensitivity troponin T concentrations in sufferers undergoing noncardiac surgical procedure: a prospective cohort examine. Incremental worth of highsensitive troponin T along with the revised cardiac index for peri-operative danger stratification in non-cardiac surgical procedure. High-sensitivity cardiac troponin T in prediction and prognosis of myocardial infarction and long-term mortality after noncardiac surgery. A meta-analysis comparing the prognostic accuracy of six diagnostic tests for predicting perioperative cardiac danger in patients undergoing major vascular surgery. A metaanalytic comparison of preoperative stress echocardiography and nuclear scintigraphy imaging. Semiquantitative dipyridamole myocardial stress perfusion imaging for cardiac danger assessment before noncardiac vascular surgery: a meta-analysis. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a potential, multicenter, multivendor research. Risk stratification using computed tomography coronary angiography in patients undergoing intermediate-risk noncardiac surgical procedure. Prognostic capabilities of coronary computed tomographic angiography before non-cardiac surgical procedure: prospective cohort examine. Systematic preoperative coronary angiography and stenting improves postoperative results of carotid endarterectomy in sufferers with asymptomatic coronary artery disease: a randomised managed trial. Risk of major adverse cardiac occasions following noncardiac surgery in sufferers with coronary stents. Association of coronary stent indication with postoperative outcomes following noncardiac surgical procedure. Anti-platelet impact of aspirin is considerably decreased after administration of heparin during carotid endarterectomy. Outcome of coronary heart failure with preserved ejection fraction in a population-based examine. The survival of patients with coronary heart failure with preserved or decreased left ventricular ejection fraction: an individual affected person information meta-analysis. Worsening preoperative coronary heart failure is associated with mortality and noncardiac issues, however not myocardial infarction after noncardiac surgical procedure: a retrospective cohort research. Perioperative outcome and long-term mortality for coronary heart failure patients present process intermediate- and high-risk noncardiac surgical procedure: influence of left ventricular ejection fraction. Perioperative diastolic dysfunction in patients undergoing noncardiac surgical procedure is an impartial threat issue for cardiovascular occasions: a scientific evaluation and meta-analysis. Echocardiography for assessing cardiac threat in patients having noncardiac surgical procedure. Usefulness of transthoracic echocardiography as a device for risk stratification of patients present process main noncardiac surgical procedure. Outcomes of sufferers with steady coronary heart failure present process elective noncardiac surgical procedure. Long-term results of a randomized managed trial analyzing the role of systematic pre-operative coronary angiography earlier than elective carotid endarterectomy in sufferers with asymptomatic coronary artery disease. Systematic technique of prophylactic coronary angiography improves long-term outcome after major vascular surgical procedure in medium- to high-risk patients: a prospective, randomized research. Usefulness of revascularization of sufferers with multivessel coronary artery illness earlier than elective vascular surgery for stomach aortic and peripheral occlusive disease. Alpha-2 adrenergic agonists for the prevention of cardiac problems amongst adults undergoing surgical procedure. Chronic beta blockade is associated with a greater end result after elective noncardiac surgery than acute beta blockade: a single-center propensity-matched cohort examine. Duration of preoperative -blockade and outcomes after major elective noncardiac surgery. Impact of beta-blocker initiation timing on mortality risk in sufferers with diabetes mellitus undergoing noncardiac surgical procedure: a nationwide population-based cohort examine. A systematic evaluate and meta-analysis on the hazards of discontinuing or not adhering to aspirin amongst 50,279 sufferers in danger for coronary artery illness. Aspirin in patients with previous percutaneous coronary intervention present process noncardiac surgical procedure. Risk of intraoperative hypotension with loop diuretics: a randomized controlled trial. The prevalence, incidence, progression, and risks of aortic valve sclerosis: a systematic evaluation and metaanalysis. A bedside scientific prediction rule for detecting average or extreme aortic stenosis. Perioperative danger of major non-cardiac surgical procedure in patients with severe aortic stenosis: a reappraisal in up to date practice. Impact of persistent superior aortic regurgitation on the perioperative outcome of noncardiac surgical procedure. Impact of extreme mitral regurgitation on postoperative outcomes after noncardiac surgical procedure. Bundle-branch block in middle-aged men: danger of problems and dying over 28 years. Complete bundle branch block as an independent predictor of all-cause mortality: report of seven,073 sufferers referred for nuclear train testing. Evaluation of risk stratification schemes for ischaemic stroke and bleeding in 182 678 sufferers with atrial fibrillation: the Swedish Atrial Fibrillation Cohort Study. Risk of stroke after surgery in sufferers with and without continual atrial fibrillation. Prevention of torsade de pointes in hospital settings: a scientific assertion from the American Heart Association and the American College of Cardiology Foundation. North American Society of Pacing and Electrophysiology/ British Pacing and Electrophysiology Group. A qualitative systematic review for the society of anesthesia and sleep drugs task pressure on preoperative preparation of sufferers with sleep-disordered respiration. Obstructive sleep apnea screening and postoperative mortality in a big surgical cohort.
|